Can MFTs Bill Medicare? Enrollment, Codes & Billing Guide
MFT Medicare Billing: How to Enroll, Bill, and Get Reimbursed
A step-by-step guide to the Medicare enrollment process, covered CPT codes, reimbursement structure, and telehealth rules for marriage and family therapists.
Licensed MFTs have been eligible to enroll as Medicare providers and bill Part B since January 1, 2024.
MFT reimbursement is set at 75% of the clinical psychologist rate under the Medicare Physician Fee Schedule.
Telehealth sessions are billable with specific modifiers, though Medicare audits telehealth claims at higher rates than in-person visits.
Over 67 million Medicare beneficiaries now represent a major new client base for MFTs in private practice, rural clinics, and hospice settings.
Yes, licensed marriage and family therapists can bill Medicare. That changed on January 1, 2024, when MFTs gained recognition as Medicare Part B providers for the first time in the program's history. The enabling legislation was Section 4121 of the Consolidated Appropriations Act of 2023, widely known as the Mental Health Access Improvement Act.
The shift matters for practical reasons. More than 67 million Medicare beneficiaries now have access to MFT services, and therapists who enroll can tap a patient population that was previously off-limits unless they worked under a physician or in a federally qualified health center. For clinicians weighing private practice viability or considering geriatric and family-focused caseloads, Medicare enrollment has become a core business decision, not an optional add-on.
The Mental Health Access Improvement Act: What Changed for Mfts
For decades, marriage and family therapists held a paradoxical position in American health care. Licensed in all 50 states, recognized by the Department of Defense and the Veterans Health Administration, and embedded in community mental health systems nationwide, MFTs were nonetheless shut out of the single largest health insurance program in the country. Medicare, which covers more than 65 million Americans, simply did not list MFTs (or licensed mental health counselors) among its approved provider types. That exclusion persisted from the program's founding in 1965 through 2023, a span of nearly six decades.
Advocacy organizations pushed corrective legislation in virtually every congressional session for more than 20 years. Bills were introduced, referred to committee, and allowed to expire, session after session. The persistence finally paid off in late 2022.
The Legislative Breakthrough
On December 29, 2022, President Biden signed the Consolidated Appropriations Act of 2023 into law. Section 4121 of that omnibus spending package amended the Social Security Act to add marriage and family therapists and licensed mental health counselors as recognized Medicare Part B provider types. The effective date was set for January 1, 2024, giving the Centers for Medicare and Medicaid Services (CMS) roughly one year to publish implementing rules and open the enrollment pathway.
This was not a standalone mental health bill. It was folded into a broader appropriations package, a common legislative strategy for provisions that carry bipartisan support but lack the political urgency to move on their own. The underlying policy language, however, drew directly from the Mental Health Access Improvement Act, a bill reintroduced repeatedly in prior sessions.
What 'Medicare Provider' Actually Means for MFTs
Beginning January 1, 2024, a licensed marriage and family therapist who completes Medicare enrollment can independently bill Original Medicare (Part B) for outpatient mental health services. The word "independently" is critical here. Unlike some provider arrangements that require physician supervision or referral, MFTs bill under their own National Provider Identifier (NPI) and receive payment directly from CMS. No supervising psychiatrist or psychologist needs to co-sign a claim.
This change opens the door to serving Medicare beneficiaries in private practice, group practices, telehealth platforms, and a range of institutional settings, significantly expanding MFT career paths across the profession.
Key Limitations to Know From the Start
The new provider status comes with two built-in constraints that every MFT should understand before enrolling:
Reimbursement rate: MFT services are reimbursed at 75 percent of the rate Medicare pays for the same service delivered by a clinical psychologist. That psychologist rate is itself lower than the psychiatrist rate, so the effective per-session payment to MFTs sits on the lower end of the Medicare fee schedule.
Mandatory assignment: MFTs must accept assignment on all Medicare claims. In practical terms, this means you agree to accept the Medicare-approved amount as full payment. You cannot balance-bill beneficiaries for any difference between your standard fee and what Medicare pays.
These limitations are not unique to MFTs. Licensed clinical social workers have practiced under comparable terms for years; for a deeper look at how the two credentials compare, see our breakdown of the difference between LMFT and LCSW. Understanding the reimbursement structure before you enroll helps you plan realistic revenue projections and decide whether Medicare participation fits your practice model.
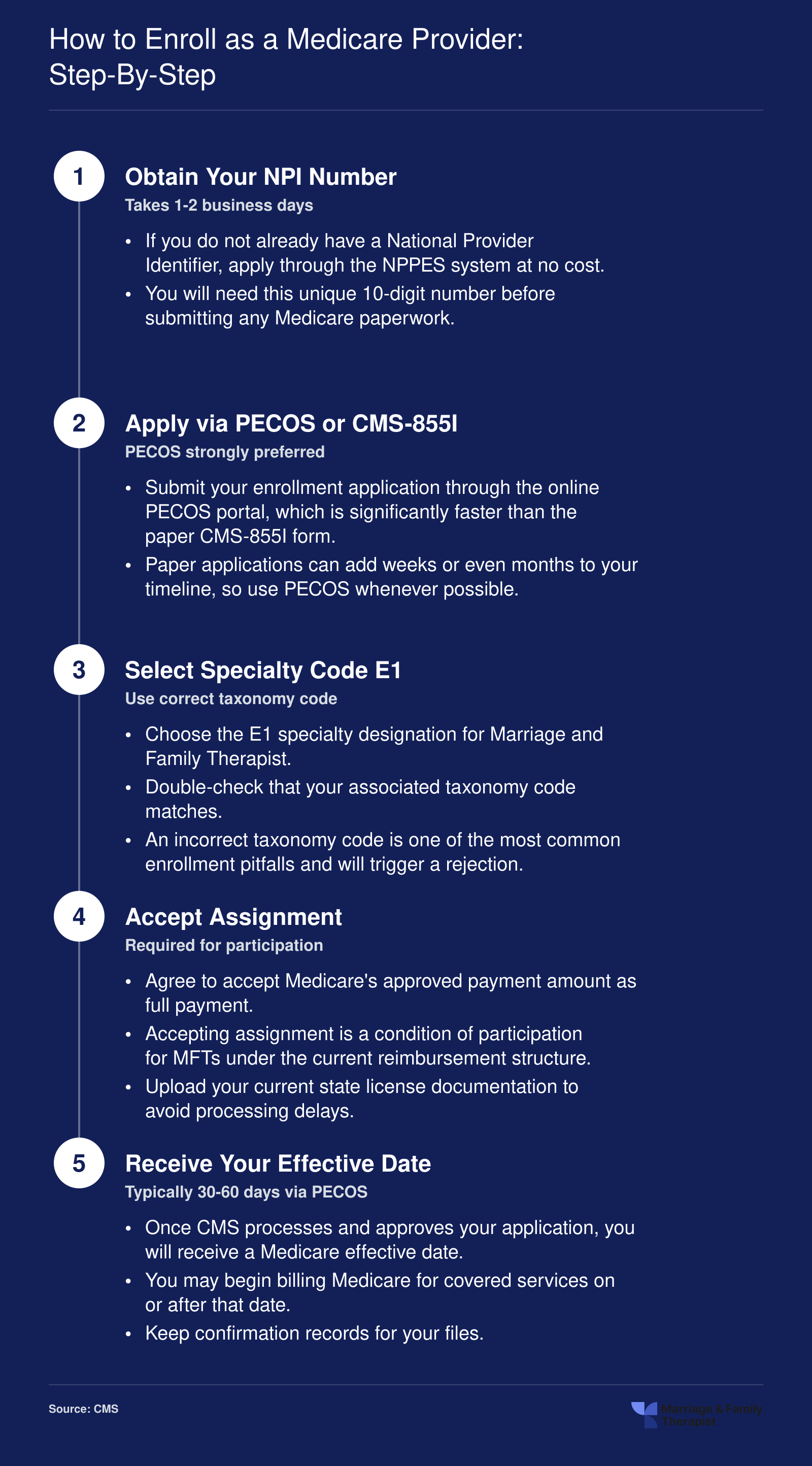
How to Enroll as a Medicare Provider: Step-By-Step
Since January 1, 2024, licensed marriage and family therapists have been eligible to enroll as Medicare providers. The process is straightforward, but incomplete applications or incorrect codes are the most common reasons for delays. Follow these five steps to get enrolled efficiently.
Medicare Enrollment for Mfts: Detailed Walkthrough
Getting enrolled as a Medicare provider involves multiple systems and a fair amount of paperwork. Rushing through any step can delay your approval by weeks or even months. Below is a detailed walkthrough covering every stage from NPI verification to your first confirmed enrollment.
Verify or Obtain Your NPI Through NPPES
Most licensed marriage and family therapists already hold a National Provider Identifier, but the first order of business is confirming that your existing NPI is active and that the information on file is accurate. Log in to the National Plan and Provider Enumeration System (NPPES) and check that your name, practice address, and taxonomy code are current. MFTs should be listed under taxonomy code 106H00000X, which corresponds specifically to marriage and family therapists. If you have never applied for an NPI, you can do so at no cost through NPPES. Processing usually takes a few business days. Without an active, correctly coded NPI, your Medicare application will stall before it even reaches a reviewer.
Complete the PECOS Application
The Provider Enrollment, Chain, and Ownership System (PECOS) is CMS's online portal for Medicare enrollment. Start by creating an Identity and Access Management (I&A) account if you do not already have one. Once logged in, you will complete the CMS-855I form, which is the individual practitioner enrollment application. Key steps include:
Specialty selection: Choose specialty code E1, which is the designation CMS created for marriage and family therapists when it began accepting MFT enrollments in 2024.
State license upload: You will need a digital copy of your current, unrestricted state license as an LMFT (or your state's equivalent credential).
Accepted assignment: Medicare requires MFTs to accept assignment on all claims. This means you agree to accept the Medicare-approved amount as full payment for covered services, and you cannot balance-bill patients beyond the standard deductible and coinsurance.
Double-check every field before submission. A single mismatch between your NPI record and PECOS application, such as a slightly different business name or an outdated address, can trigger a request for additional information and reset the processing clock.
Understand Effective Date Rules
Medicare enrollment is retroactive to the date CMS receives a complete application, not the date it finishes processing. However, the review window typically runs 60 to 90 days. During that waiting period, you should not bill Medicare for services rendered. Claims submitted before your enrollment is officially confirmed will be denied, and resubmitting them after the fact creates unnecessary administrative headaches. Plan accordingly by building your non-Medicare caseload or scheduling your enrollment well before you intend to see Medicare beneficiaries.
Common Pitfalls to Avoid
Several mistakes trip up first-time enrollees, and many guides overlook them entirely.
Wrong specialty code: Selecting a generic counseling specialty instead of E1 can result in outright denial or enrollment under a category that limits the services you can bill.
Skipping ordering and referring opt-in: If you plan to refer Medicare patients for lab work, imaging, or specialist consultations, you must separately opt in as an ordering and referring provider within PECOS. Failing to do so means your referrals will be rejected, which disrupts patient care.
Missing revalidation deadlines: CMS requires providers to revalidate their enrollment periodically (typically every five years, though the timeline can shift). If you miss a revalidation notice, your billing privileges can be deactivated without warning. Set a calendar reminder well in advance of your revalidation due date, which you can find in your PECOS account. Keeping up with LMFT continuing education requirements by state is equally important, since an expired or lapsed license will also jeopardize your Medicare enrollment.
Taking the time to complete each step carefully will save you from costly delays and ensure you can begin serving Medicare beneficiaries as soon as your enrollment is confirmed.
Questions to Ask Yourself
What percentage of your current or prospective caseload is 65 or older?
If Medicare-eligible adults make up even 15 to 20 percent of your local population, enrollment could meaningfully expand your referral base. Areas with large retiree communities offer especially strong demand for licensed therapists who accept Medicare.
Are you ready to handle Medicare's documentation and billing requirements?
Accepting assignment means agreeing to Medicare's fee schedule, submitting compliant claims, and maintaining thorough session notes. If you lack billing support or administrative staff, factor in the cost of credentialing services or practice management software before enrolling.
Could Medicare credentials unlock new employment settings you currently cannot access?
Federally Qualified Health Centers, skilled nursing facilities, hospice programs, and rural health clinics often require providers to be Medicare enrolled. Adding this credential can open salaried positions and contract opportunities that were previously off limits to MFTs.
CPT Codes Mfts Can Bill Under Medicare
Understanding which procedure codes you can submit is essential to getting paid correctly and avoiding claim denials. Below is a practical breakdown of the codes available to licensed marriage and family therapists under Medicare Part B, organized by service category.1
Individual Psychotherapy
These are the bread-and-butter codes most MFTs will bill on a daily basis. Each corresponds to a face-to-face session with the patient.
90832: Psychotherapy, 30 minutes with the patient. Use this for shorter check-in or follow-up sessions. Billable in office, facility, and telehealth settings.
90834: Psychotherapy, 45 minutes with the patient. This is the most commonly billed individual therapy code and the session length many payers consider the clinical standard.
90837: Psychotherapy, 60 minutes with the patient. Reserve this for longer, more intensive individual sessions. Documentation should support the medical necessity of the extended time.
All three codes can be billed with a place-of-service indicator for an office (11), a facility (22), or a telehealth encounter (02), which affects the reimbursement rate.
Family and Couples Therapy
Family-focused codes are especially relevant to MFTs, given the profession's systemic orientation. Clinicians exploring MFT career paths will find that these codes open the door to reimbursable conjoint and family work with Medicare beneficiaries.
90846: Family psychotherapy without the patient present. Useful when working with caregivers or family members of a Medicare beneficiary who cannot attend.
90847: Family psychotherapy with the patient present. The most straightforward family therapy code, covering conjoint sessions that include the identified patient.
90849: Multiple-family group psychotherapy. Applies when you are treating more than one family unit in a group format.
Remember that the Medicare beneficiary must be the identified patient on the claim, even when family members participate in the session.
Crisis Intervention
Crisis codes cover urgent, unscheduled psychotherapy for patients in acute distress.
90839: Psychotherapy for crisis, first 60 minutes. Bill this when a patient presents with an urgent behavioral health crisis requiring immediate intervention.
90840: Each additional 30 minutes of crisis psychotherapy. This is an add-on code, meaning it can only be billed alongside 90839. If the crisis session extends beyond the initial hour, append 90840 for each qualifying 30-minute block.
Behavioral Health Integration
These codes apply when MFTs participate in collaborative or integrated care models, often within primary-care or team-based settings.
G0323: Care management services for behavioral health conditions. This code supports ongoing behavioral health care coordination.
99492: Initial psychiatric collaborative care management for the first month of treatment. Used when the MFT serves as the behavioral health manager in a collaborative care arrangement.
99493 and 99494: Subsequent monthly collaborative care management and add-on services, respectively.
Behavioral health integration codes are particularly relevant for MFTs working in federally qualified health centers, rural health clinics, and other team-based environments.
Add-On Codes Worth Knowing
Beyond the primary service codes, MFTs should be aware of one frequently applicable add-on.
+90785: Interactive complexity. Append this to any psychotherapy code when the session involves factors that complicate delivery, such as the use of an interpreter, involvement of a third party (like a guardian), or the need to manage disruptive communication patterns during a family session. It cannot be billed on its own.
Keeping a quick-reference sheet of these codes, along with their time thresholds and place-of-service rules, can streamline your billing workflow and reduce the likelihood of rejected claims. For a deeper look at how reimbursement rates attach to each of these codes, continue to the next section.
MFT Medicare Reimbursement Rates Explained
Understanding how Medicare pays marriage and family therapists is essential before you build a caseload around Medicare beneficiaries. The reimbursement formula is straightforward, but the dollar amounts vary by service code and geographic location, so running the numbers for your area is a critical step.
The 75 Percent Formula
Under the Medicare Physician Fee Schedule (MPFS), clinical psychologists are reimbursed at 100 percent of the schedule amount for a given CPT code. MFTs, by contrast, receive 75 percent of the psychologist rate.1 This discount mirrors the structure Congress established in the Mental Health Access Improvement Act and is consistent with how Medicare has historically tiered non-physician providers.
Using 2026 national (non-facility) rates, here is what the math looks like for the three codes MFTs bill most often:2
90834 (Individual therapy, 45 min): The psychologist rate is approximately $134.25. At 75 percent, the MFT rate comes to roughly $85.43 per session.
90837 (Individual therapy, 53+ min): The psychologist rate is approximately $172.80, putting the MFT rate near $125.25.
90847 (Family therapy with patient present): The psychologist rate is approximately $145.60. The MFT rate lands around $82.16.
Family therapy codes may reflect a steeper effective discount depending on the specific conversion factor and relative value units assigned by CMS in a given year. Always verify current rates on the CMS fee schedule lookup tool before quoting fees to patients.
Geographic Variation: Location Matters
Medicare adjusts every fee through Geographic Practice Cost Indices (GPCIs), which account for differences in practice expense, malpractice cost, and provider work value across localities. The gap between a high-cost metro and a rural area can be significant.
For CPT 90834, consider these approximate 2026 MFT rates:1
Manhattan, New York: roughly $116 to $117 per session
National average: roughly $85 per session
Rural Texas: roughly $92 to $93 per session
Manhattan's elevated cost index pushes reimbursement well above the national figure, while rural Texas falls closer to, and sometimes slightly above, the national baseline because of GPCI adjustments specific to that locality. If you are evaluating where to open a practice or whether to accept Medicare patients, pulling the locality-specific rates for your county is a practical first step.
What You Actually Collect: The 80/20 Split
Medicare does not pay the full allowed amount out of its own pocket. Under Original Medicare (Part B), the program covers 80 percent of the approved fee. The remaining 20 percent is the patient's responsibility, typically collected as a copay or covered by a Medigap supplemental plan.
Using the national MFT rate for a 45-minute individual session (CPT 90834) as an example:
Total allowed amount: approximately $85.43
Medicare pays (80 percent): approximately $68.34
Patient copay (20 percent): approximately $17.09
You still collect the full allowed amount across those two sources, but cash flow timing differs. Medicare's portion arrives through electronic remittance within roughly two to four weeks. The patient copay must be billed and collected by your office. If a patient also has Medicaid as a secondary payer or carries a Medigap policy, the copay may be covered automatically, simplifying collections.
The Financial Reality for Private Practice
At roughly $85 per 45-minute session or $125 per extended session at the national average, Medicare rates for MFTs are lower than what many therapists charge private-pay clients. That said, these rates are guaranteed and backed by federal payment infrastructure, which reduces the uncertainty of building a caseload. For MFTs in settings such as Federally Qualified Health Centers, skilled nursing facilities, or rural health clinics, Medicare patients can represent a reliable revenue stream that supplements other payer mixes.
The key is to treat the MPFS rate as a floor, not a ceiling. You can still maintain a blended caseload of Medicare, commercial insurance, and private-pay clients, adjusting your panel size to hit your income targets. Our ROI analysis of an MFT degree offers additional context on what licensed MFTs earn across practice settings, helping you model realistic revenue projections before you commit to Medicare enrollment.
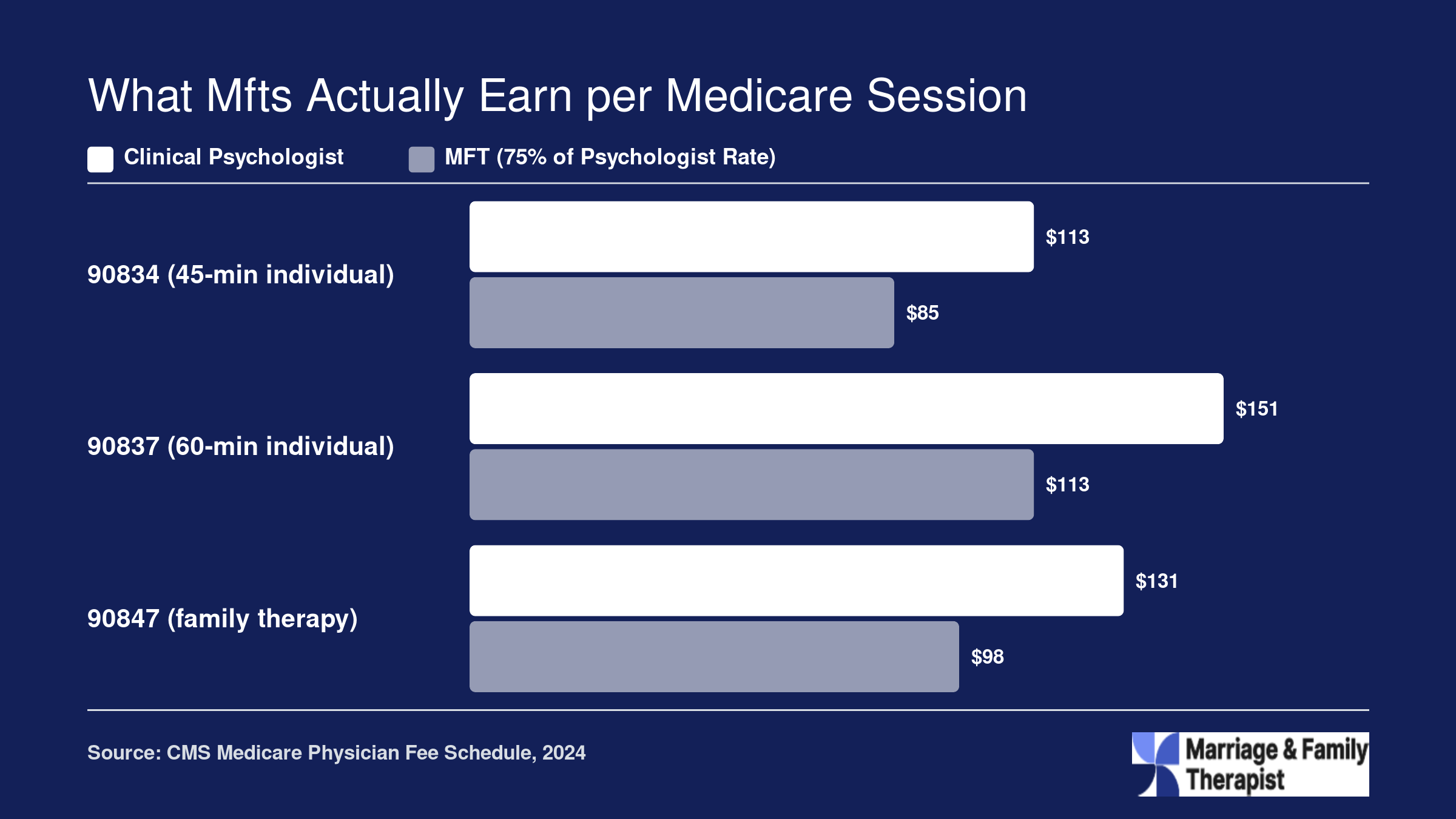
What Mfts Actually Earn per Medicare Session
Under the Medicare Physician Fee Schedule, licensed marriage and family therapists are reimbursed at 75% of the rate paid to clinical psychologists for the same CPT codes. The figures below reflect 2024 national non-facility rates before the standard 80/20 coinsurance split (Medicare pays 80%, the patient owes 20%). Keep in mind that geographic locality adjustments can shift these amounts by 10% to 20% depending on where you practice.
Telehealth Billing Rules for Mfts Under Medicare
Licensed marriage and family therapists have been eligible to deliver and bill for telehealth services under Medicare since January 1, 2024.1 If you plan to see Medicare beneficiaries via video or phone, you need to understand the modifiers, place-of-service codes, and originating-site rules that govern reimbursement. Getting these details right prevents claim denials and keeps your practice compliant.
Video Telehealth: Modifier 95 and Place-of-Service Codes
When you provide a synchronous, real-time audio-video session, append modifier 95 to your CPT code. This is the current standard modifier for live video telehealth across all Medicare Administrative Contractors (MACs). Some MACs historically required the legacy GT modifier instead; if your MAC still requests GT, follow its guidance, but modifier 95 is the default for 2026 billing.1
You also need the correct place-of-service (POS) code on each claim:
POS 10: Use this when the patient is joining the session from their home.
POS 02: Use this when the patient is located at any site other than their home, such as a clinic, community center, or assisted-living facility.
Selecting the wrong POS code is one of the most common reasons telehealth claims are returned, so verify the patient's location at the start of every session and document it.
Audio-Only Sessions: Permanent and Extended Provisions
Medicare permits MFTs to bill certain services delivered by telephone alone. For behavioral health codes, audio-only billing is a permanent allowance, meaning it does not expire.1 For non-behavioral-health codes, the audio-only option has been extended through December 31, 2027.1
Eligible audio-only CPT codes for MFTs include 90791, 90832, 90834, 90837, 90846, 90847, and 90853.2 Append modifier 93 to indicate the service was furnished via audio-only technology. Your documentation must explain why video was not feasible or why the patient preferred a phone session, and you should note that the patient consented to the audio-only format.
Originating-Site and Geographic Restrictions
Before the pandemic-era flexibilities, Medicare limited telehealth to patients in designated rural areas who presented at an approved originating site such as a hospital or clinic. Those geographic and facility-type restrictions have been waived, and the waiver remains in effect through December 31, 2027.1 That means your Medicare patients can receive telehealth from anywhere in the country, including their own homes, with no rural-area requirement.
CMS has also deferred the proposed in-person visit requirement that would have mandated a face-to-face encounter within six months of a telehealth-only relationship. As of 2026, no such mandate is being enforced, though you should monitor future rulemaking cycles for changes.1
Practical Documentation Tips
Every telehealth encounter should include:
The patient's physical location and state at the time of service.
The technology used (audio-video or audio-only) and the reason if audio-only.
Verbal or written patient consent for telehealth.
Start and stop times, consistent with time-based CPT code requirements.
Federally Qualified Health Centers and Rural Health Clinics also retain the ability to bill Medicare for MFT telehealth services through 2026 under extended payment provisions, making these settings especially viable for therapists building telehealth-heavy caseloads.1 Therapists exploring whether the MFT degree is worth the investment should factor in this expanded telehealth access, which significantly broadens the pool of reimbursable clients.
Staying current with CMS telehealth policy is essential. The flexibilities MFTs enjoy right now are generous, but many carry a 2027 sunset date. Maintaining compliant LMFT continuing education requirements by state and building sound billing habits today protects your revenue and positions your practice to adapt smoothly if rules tighten.
Medicare telehealth claims are audited at higher rates than in-person visits, making thorough documentation essential. For every telehealth session, record the modality (video or audio only), the patient's location at the time of service, your clinical rationale for delivering care remotely, and confirmation that the patient provided verbal consent. Missing any of these details is one of the most common denial triggers for new MFT Medicare billers.
Billing in Special Settings: Snfs, Rhcs, Fqhcs, and Hospice
Medicare billing for marriage and family therapists does not look the same in every clinical environment. If you plan to work in a skilled nursing facility, a rural or community health center, or a hospice program, you need to understand how reimbursement mechanics shift from one setting to the next. Each facility type operates under its own Medicare payment model, and knowing the rules before you accept a position or sign a contract can save you significant revenue headaches.
Skilled Nursing Facilities (SNFs)
SNFs bundle most services into a single per-diem payment under the Prospective Payment System, but MFT services are excluded from that consolidated billing bundle.1 This is the same carve-out that already applied to psychologists and clinical social workers. In practical terms, the exclusion means you can bill Medicare Part B directly for therapy sessions you provide to SNF residents rather than routing claims through the facility.1 You submit claims under your own NPI just as you would in an outpatient office. This makes SNFs a particularly attractive employment or contracting opportunity because your reimbursement does not depend on the facility's internal accounting.
Rural Health Clinics and Federally Qualified Health Centers
RHCs and FQHCs now recognize MFTs as covered behavioral health providers.2 However, billing here works differently from standard fee-for-service claims. RHCs use an all-inclusive rate per visit, while FQHCs operate under their own Prospective Payment System.3 Neither setting reimburses based on individual CPT codes. Instead, each qualifying face-to-face encounter generates one bundled payment to the facility. You will not see line-item reimbursement for a 90837 or 90834 the way you would in private practice.
For MFTs, the key practical difference is that the clinic, not you, submits the claim and receives the payment. Your compensation comes through your employment or contractor agreement with the facility. MFTs in these settings can also participate in the Collaborative Care Model, which can further expand the types of patients you serve.2
Hospice Programs
MFTs can serve as counselors on a hospice interdisciplinary team, providing bereavement and family counseling that is central to end-of-life care.4 Billing mechanics here differ substantially from other settings. Counseling services are bundled into the hospice per-diem rate, meaning you bill through the hospice provider rather than independently under your own NPI.4 If you do treat a hospice patient for a condition that is unrelated to the terminal diagnosis, you may bill Part B separately, but you must clearly document that the services address a distinct, unrelated condition.
Group Practice Considerations
MFTs working in group practice settings should bill Medicare directly under their own NPI.5 Although incident-to billing exists as a framework for certain allied health professionals, it is not recommended for MFTs.5 Incident-to rules impose supervision and documentation requirements that can create compliance risk and may not align with your scope of practice as an independently licensed provider. Billing under your own number is cleaner, reduces audit exposure, and ensures that your services are attributed correctly in Medicare's records. If a group practice employer asks you to bill under a physician's NPI, consult a healthcare billing specialist before agreeing to that arrangement.
Understanding these setting-specific rules positions you to pursue a wider range of marriage and family therapist job outlook opportunities, from geriatric care in nursing facilities to underserved-community work in FQHCs, without leaving reimbursement on the table.
Common Medicare Claim Denials for Mfts and How to Appeal
Even well-prepared MFTs run into claim denials during their first months as Medicare providers. Understanding why claims get rejected, and knowing how to fix and appeal them, saves you weeks of lost revenue and frustration.
Most Frequent Denial Reasons for New MFT Providers
The denials that hit newly enrolled MFTs hardest tend to fall into a handful of predictable categories:
Enrollment not yet active at date of service: Medicare only pays for services rendered on or after your assigned effective date. If you submit a claim for a session that took place before your enrollment was fully processed, it will be denied outright.1
Incorrect specialty or taxonomy code: Your NPI must be linked to the correct MFT taxonomy. A mismatch between your provider type and the specialty code on the claim triggers an automatic rejection.
Missing or incorrect modifier: Telehealth sessions, for example, require modifier 95 or GT. Omitting the modifier or using the wrong one is one of the most common errors in the first billing cycle.2
Insufficient medical necessity documentation: Medicare requires documentation that treatment is expected to produce improvement or prevent deterioration. Notes should follow a SOAP or DAP structure and include the diagnosis, measurable goals, interventions used, and session time.1
Non-covered diagnosis codes: Relationship problems billed under Z codes alone are not covered. Medicare requires an F-code diagnosis from the DSM-5 to establish medical necessity. Maintenance therapy without a documented expectation of improvement or prevention of decline is likewise not covered.1
Understanding the Denial Codes You Will See
When a claim is denied, Medicare returns adjustment reason codes that tell you what went wrong.3 Three codes appear frequently for MFT providers:
CARC 16: This means the claim or service lacks the information needed for adjudication. It usually points to a missing modifier, an incomplete field, or incorrect provider data.4
CO-4: This code indicates the procedure or revenue code is inconsistent with the modifier used or missing a required modifier entirely.
CO-109: This signals that the claim is not covered by the payer or plan, often because the diagnosis code is excluded from Medicare coverage (such as a standalone Z code).
Reading these codes carefully before resubmitting prevents repeated denials for the same issue.
How the Medicare Appeals Process Works
Medicare has a five-level appeals system, but the vast majority of MFT denials are resolved at the first level.
The first level is called a redetermination. You file it using CMS form 20027, and you must submit the request within 120 days of the denial notice. Include corrected documentation, a brief explanation of the error, and any supporting records. The Medicare Administrative Contractor is required to issue a decision within 60 days.
If the redetermination does not resolve the issue, the second level is a reconsideration filed on CMS form 20033 within 180 days. Beyond that, further levels include an Administrative Law Judge hearing, Medicare Appeals Council review, and ultimately federal district court. In practice, most MFT denials stem from correctable data errors and are overturned at redetermination.
Practical Steps to Prevent Denials Before They Happen
Prevention is far easier than appeals. Before you submit your first claim, take the following steps:
Verify your enrollment effective date in the PECOS system and do not bill for any service provided before that date.1
Run patient eligibility checks before every session to confirm active Medicare coverage.
Double-check your place-of-service code, especially when alternating between in-person and telehealth visits.
Document every session with a DSM-5 F-code diagnosis, clear treatment goals, specific interventions, and the total time spent.
Create a denial tracking log from day one. Recording each denial reason, the correction you made, and the outcome builds a reference that helps you and your billing staff spot patterns quickly.6
Claim denials are a normal part of the learning curve for any new Medicare provider. Therapists who understand what an MFT does in clinical practice already have a strong foundation for translating their work into compliant documentation. Approach denials systematically, correct the root cause rather than simply resubmitting, and most issues will resolve themselves before you ever need to file a formal appeal.
Medicare Advantage Vs. Original Medicare: What Mfts Need to Know
Understanding the difference between Original Medicare and Medicare Advantage (MA) plans is critical for any MFT building a sustainable practice. More than half of all Medicare beneficiaries are now enrolled in MA plans, which means ignoring this side of the market could cut you off from the majority of potential clients.
How Original Medicare Works for MFTs
Original Medicare (Parts A and B) is administered directly by the Centers for Medicare and Medicaid Services.1 Once you complete your CMS enrollment, you can bill Medicare directly for covered services. Reimbursement rates are set by the Medicare Physician Fee Schedule at 75 percent of the rate paid to psychologists for comparable services.2 There is no network to join and no additional contracting step; your CMS enrollment is your credential.
How Medicare Advantage Differs
MA plans are offered by private insurers that contract with CMS. By law, every MA plan must cover at least everything Original Medicare covers, so MFT services should be included as a Part B benefit.3 However, the similarities largely end there:
Credentialing: Each MA plan runs its own credentialing and contracting process, separate from your CMS enrollment. You may need to apply to dozens of plans depending on your region.
Reimbursement rates: MA plans negotiate their own fee schedules. Rates are not automatically pegged to 75 percent of the psychologist rate; they could be higher or lower depending on the contract you sign.
Network requirements: Most MA plans use provider networks. If you are not credentialed with a specific plan, beneficiaries enrolled in that plan generally cannot see you for covered services, or they will face higher out-of-pocket costs.
Billing pathway: You do not bill CMS directly. Instead, claims go to the MA plan, and each plan may have its own submission rules, prior-authorization requirements, and timelines.
Why MA Credentialing Matters for Practice Viability
Because over half of Medicare beneficiaries now choose MA plans, completing only your CMS enrollment leaves a significant gap in your potential caseload. If you plan to serve older adults, whether in private practice, a community clinic, or a rural health setting, credentialing with the major MA plans in your area is essentially non-negotiable. Start the process early; MA credentialing timelines vary by insurer and can take several months. Understanding how LMFT vs psychologist reimbursement differs can also help you benchmark the rates MA plans offer during contract negotiations.
The bottom line: enroll with CMS first to establish your Original Medicare billing ability, then systematically credential with the MA plans that dominate your local market. Covering both pathways positions you to serve the full spectrum of Medicare beneficiaries walking through your door.
What MFT Medicare Coverage Means for Your Career
The ability to bill Medicare is not just a billing update. It is a structural shift in how marriage and family therapists can build, sustain, and grow their careers. With more than 67 million Americans currently enrolled in Medicare, and the 65-plus population projected to keep expanding for the next two decades, MFTs now have direct access to the fastest-growing client demographic in the country.
A Viable Path to Private Practice
Before 2024, MFTs who wanted to open a private practice had to rely entirely on commercial insurance panels and private-pay clients. That narrowed the potential client base and made revenue unpredictable. Medicare enrollment changes that equation. Adding Medicare to your payer mix means you can accept referrals from hospitals, primary care physicians, and senior centers that previously could not send patients to an MFT for reimbursable care. The result is a more diversified, more resilient income stream. If you are weighing salary expectations as you plan your career, understanding what Medicare reimbursement adds to the picture is essential.
Expanded Hiring Opportunities
Federally Qualified Health Centers, rural health clinics, skilled nursing facilities, and settings adjacent to the VA system are actively recruiting licensed marriage and family therapists who can bill Medicare. These organizations serve large Medicare populations and need clinicians who are already credentialed with the program. For job seekers, Medicare eligibility makes your resume significantly more competitive, especially in underserved and rural areas where provider shortages are acute. Those exploring the full marriage and family therapist job outlook will find that many of the most in-demand positions now list Medicare billing capability as a preferred or required qualification.
Geriatric and Family Systems Caseloads
Medicare-eligible clients frequently present with concerns that sit squarely within an MFT's core competency. Caregiver burnout, grief after the loss of a spouse, adjustment to chronic illness, and family conflict around end-of-life planning are all issues that benefit from a family systems approach. Clinicians trained in medical family therapy are especially well positioned to address the intersection of physical health and relational dynamics in this population. MFTs are uniquely equipped to treat the individual within the context of relationships, making them well suited for the complex psychosocial needs of older adults and their families.
Plan Ahead if You Are Still in Training
Aspiring MFTs should factor Medicare billing into their career planning from the start. Choosing a COAMFTE-accredited program, accumulating supervised clinical hours with geriatric populations, and learning the basics of insurance credentialing during graduate school will position you to enroll as a Medicare provider soon after licensure. Understanding the AMFT to LMFT timeline can help you map out when you will be eligible to apply for your own Medicare credentials. Treat Medicare readiness as part of the licensure roadmap, not an afterthought.
The bottom line: Medicare access transforms the MFT credential from a license with limited insurance reach into one that can serve virtually every age group, in nearly every clinical setting, with a federally backed reimbursement guarantee. That is a career game-changer by any measure.
Frequently Asked Questions About Mfts and Medicare
Below are answers to the questions marriage and family therapists ask most often about Medicare enrollment, billing, and reimbursement. Each answer reflects the rules in effect as of 2026.
Can marriage and family therapists bill Medicare?
Yes. As of January 1, 2024, fully licensed marriage and family therapists are recognized Medicare providers and may bill the program directly under their own NPI. You must hold state licensure with independent practice authority, possess a master's degree or higher, and have completed the required supervised clinical experience. Pre-licensed or associate-level clinicians are not eligible.
What is the Mental Health Access Improvement Act?
Signed into law in December 2022, the Mental Health Access Improvement Act added licensed marriage and family therapists (and licensed professional counselors) to the list of Medicare-recognized providers. The law took effect January 1, 2024, allowing MFTs to enroll in Medicare, submit claims, and receive reimbursement for covered psychotherapy and evaluation services for the first time.
How much does Medicare reimburse MFTs per session?
Medicare pays MFTs at 75% of the Physician Fee Schedule rate for each covered CPT code. For a standard 45-minute individual psychotherapy session (CPT 90834), that typically falls in the range of roughly $80 to $100 before any geographic adjustments. Exact amounts vary by locality, and the rates are updated each calendar year through the Medicare Physician Fee Schedule Final Rule.
Do Medicare Advantage plans cover MFT services?
Medicare Advantage (Part C) plans must cover at least the same services as Original Medicare. Because Original Medicare now covers MFT services, Medicare Advantage plans are required to include them as well. However, each plan sets its own provider networks, copay structures, and prior authorization rules, so MFTs should verify terms with individual insurers before treating enrollees.
Can associate-level or pre-licensed MFTs bill Medicare?
No. As of 2026, only fully licensed MFTs with independent practice authority in their state may enroll as Medicare providers and bill under their own NPI. Pre-licensed clinicians, associates, and those practicing under supervision cannot submit Medicare claims independently. They must first complete all licensure requirements before applying for Medicare enrollment through PECOS.
What documentation does Medicare require for MFT services?
Medicare requires an initial evaluation, a written treatment plan, and progress notes for every service billed. Treatment plans must include the ICD-10-CM diagnosis, measurable goals, planned interventions, session frequency, and expected duration. Each progress note must document the date of service, CPT code, session type, participants present, presenting symptoms, interventions used, the client's response, a risk assessment, and the ongoing plan.
Can MFTs bill Medicare for couples therapy?
It depends. Medicare covers family psychotherapy (CPT 90847) only when the identified patient is the Medicare beneficiary who has a diagnosable mental health condition, and the involvement of a family member or spouse is medically necessary for treatment. Pure marital or relationship counseling without an underlying mental health diagnosis is excluded. Always assign an appropriate ICD-10-CM code that supports medical necessity.