JD Vance's therapy non-response, contrasted with his later religious conversion, underscores the importance of client-therapist fit.
AAMFT ethics require respecting client autonomy when faith is prioritized, while exploring spiritual supports without coercion.
Faith-integrated therapy shows large combined effect sizes (0.74) for spiritual and psychological outcomes, per a 2018 meta-analysis.
An estimated 27-33% of U.S. adults experience religious trauma, making spiritual competence essential for safe MFT practice.
"Therapy didn't work for you; church does," Usha Vance told Vice President JD Vance, according to a CBS News Sunday Morning interview that aired on June 14, 2026.1 The remark crystallizes a scenario marriage and family therapists face with increasing regularity: clients who trust faith communities more than clinical treatment.
Surveys show roughly one-third of Americans prefer turning to clergy for mental health support before a therapist. For MFTs, this is not a fringe concern; it is a core ethical challenge. Navigating religious skepticism means discerning when a client's rejection of therapy signals a worldview rather than a treatment-fit problem.
Licensure boards and the AAMFT Code of Ethics now explicitly require spiritual and religious competence as part of multicultural practice. The profession's ability to meet clients through varied MFT career paths, whether a client finds grounding in a pew or on a cushion, directly shapes treatment retention and outcomes.
Why Some Clients Prefer Faith Over Therapy: The Vance Example and Beyond
The Vance Case: A Clinical Vignette
When Usha Vance observed that therapy "didn't work for you; church does," she crystallized a dynamic marriage and family therapists (MFTs) encounter regularly. Her husband, Vice President JD Vance, has spoken openly about a chaotic youth marked by caregiver turnover, trauma, and an inability to develop "the right kind of trust" in the therapeutic process. After years of identifying as an atheist, he converted to Catholicism in 2019 and now describes that structured faith community as the stabilizing force therapy was not. Without diagnosing, this high-profile example mirrors a pattern many clinicians see: a client finds in religious practice the containment, moral clarity, and relational continuity that talk therapy failed to provide.
What the Pattern Teaches Us
Vance's trajectory is not unique. Research on therapy attrition repeatedly finds that client-therapist mismatch, cultural insensitivity, and worldview clashes drive early termination. For individuals whose primary attachment style responds better to communal belonging than to dyadic introspection, a religious congregation's liturgy, shared narratives, and intergenerational support can feel more reparative than weekly 50-minute sessions. Structured belief systems offer predictable roles, rituals, and answers that may soothe what feels chaotic in a client's internal world. When a therapist neglects to explore these deeper meaning-making frameworks, the client may silently exit and seek stability elsewhere. Expanding fluency across therapy approaches used by MFTs equips clinicians to meet clients where their worldview actually lives.
Common Reasons Clients Choose Faith Over Therapy
Distrust of secular authority figures: Many clients come from communities where mental health professionals are viewed as cultural outsiders who undermine faith, not helpers who respect it.
Pathologizing narratives: In some religious traditions, therapy is framed as characterizing spiritual struggles as disorders, leading clients to fear being labeled or shamed.
Concrete social support: A faith community delivers meals during a crisis, visits the sick, and surrounds a struggling family with tangible care, support that weekly therapy alone cannot replicate.
Prior negative therapy experiences: A client who once felt judged, misunderstood, or pressured to abandon religious beliefs may decide that faith offers a safer harbor.
Clinical Takeaway: Worldview Over Outcomes
A client's preference for faith over therapy is not a treatment failure, it is data. It signals a worldview in which transcendent meaning, communal belonging, and moral coherence carry more weight than insight alone. Competent MFTs receive this as vital clinical information, not a rejection of the profession. Integrating that data means asking, "How does your faith hold this pain?" or "What does your tradition say about healing?" Dismissing the client's religious resources or positioning therapy as superior erodes the alliance. Instead, therapists who can honor the client's spiritual anchoring, even while practicing within ethical boundaries, open the door for a collaborative relationship where both faith and therapeutic change can coexist.
Understanding Religious Skepticism Toward Therapy Across Faith Traditions
How do religious beliefs influence whether clients seek therapy or turn to faith leaders instead? The answer varies widely across traditions, and for marriage and family therapists, recognizing these differences is essential for building effective alliances. The Vance story, spanning Usha's Hindu upbringing and JD's conversion to Catholicism, underscores how interfaith dynamics can complicate help-seeking, especially when one partner finds healing in a faith that the other does not share.
The Catholic Context: Affirming Therapy with a Preference for Clergy First
Catholics tend to hold moderate help-seeking attitudes, often consulting a priest before a mental health professional.1 A 2023 U.S. Conference of Catholic Bishops review of 144 studies notes that while official teaching explicitly affirms secular psychotherapy and medication, some lay Catholics still believe mental health care is incompatible with faith.2 A small Irish study found that all 15 priests surveyed held positive attitudes toward mental health help, suggesting clergy often encourage rather than block treatment.1 For MFTs, this means a Catholic client may appear open yet also seek a therapist who respects the role of faith in healing.
Evangelical Protestant Patterns: Prayer and Pastoral Care Over Talk Therapy
Evangelical Protestants frequently show moderate to low help-seeking for talk therapy, with prayer or pastoral counseling as their first preference and medication accepted more readily than secular psychotherapy.1 Senior Baptist pastors have rated medications as more effective than counseling but less effective than pastoral care.1 This hierarchy can create resistance: couples may dismiss therapy because their faith community frames it as a lesser solution. MFTs who fail to acknowledge this spiritual authority can appear dismissive, while those who collaborate with couples therapist requirements may gain credibility.
Hindu and Muslim Perspectives: Family Honor, Stigma, and Traditional Healers
Both traditions exhibit low to moderate therapy utilization, with people typically turning to family, imams, temple rituals, or traditional healers first.1 In collectivist communities, external disclosure of family struggles can feel like a betrayal of self-sufficiency, threatening family honor. The Vance example is salient here: Usha was raised Hindu, JD later embraced Catholicism, and the couple's interview reveals how faith became their refuge after therapy fell short. For MFTs working with Hindu or Muslim clients, understanding these deep-rooted concerns around confidentiality and community judgment is critical to avoid reinforcing stigma.
LDS Communities: Bishops Alongside Therapists
Latter-day Saints show moderate to high therapy help-seeking, often consulting a bishop first but also engaging mental health professionals.1 The LDS model integrates ecclesiastical support with clinical care, positioning the bishop as a first-line counselor. This can ease entry into therapy but also requires MFTs to navigate dual loyalty, collaborating with faith leaders rather than competing.
What This Means for MFTs: Denominational Literacy as a Clinical Competency
Research consistently shows that higher religiosity correlates with more negative attitudes toward psychotherapy, and that Christians generally prefer therapists who share their religion, race, and sexual orientation more so than religiously unaffiliated individuals do.3 When clients expect faith or pastoral care to be sufficient, willingness to seek psychotherapy drops sharply.1 For MFTs, this is not mere courtesy; it is a clinical necessity. Knowing what a client's faith tradition teaches about suffering, healing, and authority directly shapes the therapeutic alliance. Without this literacy, therapists risk misinterpreting resistance, alienating clients, or missing opportunities to collaborate with religious leaders. The Vance narrative illustrates the ultimate risk: a client's past negative therapy experience, combined with a faith community's promise of healing, can lead to complete rejection of the profession. MFTs must proactively explore clients' worldviews, respect sacred frameworks, and, when appropriate, bridge the gap by working alongside trusted clergy.
When a client says 'I don't believe in therapy,' they express a worldview; 'Therapy hasn't worked for me' signals a treatment-fit issue. Listen for this difference. It determines whether you explore values or repair trust, and it shapes the entire therapeutic path.
AAMFT Ethics and Scope of Practice When Faith and Therapy Conflict
When clients choose faith over therapy, MFTs face an ethical intersection. The AAMFT Code of Ethics (2015) provides specific guidance to navigate these moments without compromising professional integrity or client dignity.1
Client Autonomy and the Right to Refuse Treatment
The AAMFT Code of Ethics (2015) is clear: clients have the right to make autonomous decisions about their care, including declining or discontinuing therapy.1 This principle, rooted in the profession's respect for self-determination, means that when a client asserts that church or religious practice is their preferred path, the therapist must honor that choice without coercion. Informed consent standards further require that clients be fully aware of their options, including the option to not receive therapy, before any treatment begins.
Competence Boundaries and Referral Requirements
MFTs are ethically bound to practice only within their areas of competence.1 The Code explicitly prohibits therapists from stepping into roles, such as religious counseling, for which they lack training. If a client's needs center on integrating faith in ways beyond the therapist's skill, referral is not just advisable; it is mandatory.1 The non-discrimination clause ensures that religious identity is never a basis for refusing service, but it does not compel a therapist to provide care that falls outside their professional scope. In cases of faith-based conflict, the therapist must facilitate a warm referral to a qualified professional, which might be an MFT with spiritual competence or a clergy member who respects therapeutic boundaries.
Ethical Skepticism and the Duty of Care
The term "ethical skepticism" in this context does not mean doubting a client's faith. Rather, it describes the therapist's responsibility to apply clinical discernment to all claims, including religious ones, while fully respecting the client's worldview. For example, if a client believes that prayer alone will resolve severe depression, the therapist must not dismiss that belief but should gently explore its impact and share evidence-based options. The ethical tension emerges here: how to inform without infringing on autonomy. The Code's emphasis on beneficence requires MFTs to provide relevant information, yet the dignity of the person demands that the final choice rests with the client.1 Walking this line means balancing professional knowledge with profound cultural humility.
Three Ethical Guardrails
When therapy is declined in favor of religious support, MFTs can maintain integrity through concrete steps:
Document the decision: Record the client's expressed preference for faith-based support and the therapist's offer to remain available. This protects both parties and clarifies the clinical rationale.
Leave the door open: Explicitly communicate that the therapeutic relationship can resume if circumstances change, and provide contact information without pressure. This respects autonomy while preserving safety.
Maintain neutrality on beliefs: The Code prohibits both disparaging and endorsing specific religious doctrines.1 Therapists must refrain from promoting one faith tradition over another or making evaluative statements about the client's spiritual commitments. The goal is to honor the client's framework as a source of strength while safeguarding the professional role.
These guardrails help MFTs navigate the complexity of faith-and-therapy conflicts without abandoning their ethical obligations. A revision of the AAMFT Code announced for 2026 may offer further clarity,2 but the current standards already provide a strong foundation.
When One Partner Wants Faith-Based Therapy and the Other Doesn't
When one partner seeks faith-based therapy and the other resists, the MFT must navigate a delicate line between spiritual alignment and therapeutic neutrality. This dynamic is now on public display through JD Vance's hopes that his wife Usha will convert to Christianity, a stance that can mirror private tensions MFTs encounter in session. For couples where religion carries high stakes, the therapist's role is not to resolve theological differences but to keep the relationship safe and functional despite them.
The Relational System Above Individual Worldviews
MFTs are trained to serve the relational system, not one partner's religious commitments. When faith preferences clash, the therapist must balance both partners' autonomy without endorsing a particular belief. This can be challenging if one partner frames therapy as spiritual growth and the other sees it as secular problem-solving. The Vance example highlights how even offhand remarks about conversion can create a power imbalance that mirrors in-session dynamics where one partner's faith tradition holds explicit authority over family decisions.
Strategy One: Establish Neutral Ground Rules
From the first session, set clear expectations that neither partner's belief system will serve as the default framework. This means avoiding language that favors one religious perspective, even inadvertently, and framing therapeutic goals in terms both partners can endorse. For example, instead of asking how their faith can heal the marriage, ask what strengths each draws from their separate traditions and how those strengths can support the relationship. This approach can defuse reactive positions and keep the conversation on shared objectives like better communication or healthier conflict patterns.
Strategy Two: Use Values-Mapping Exercises
Values-mapping helps couples identify common ethical ground beneath doctrinal differences. Ask each partner to articulate five core personal values, then look for overlap. A Christian spouse might list compassion, while a Hindu partner might prioritize ahimsa (non-harm); both translate practically into kindness within the home. By focusing on lived values rather than abstract theology, MFTs shift the dialogue from conversion pressures to actionable relationship commitments. This technique honors each partner's worldview while building a collaborative third space neither partner owns. Narrative therapy techniques offer a complementary path here, helping each spouse author their own story of shared values rather than competing doctrines.
Strategy Three: Address Power Dynamics Directly
When one partner's faith tradition grants them authority over family decisions, the MFT must name that power gently but firmly. For instance, if a spouse believes their religion requires them to lead the home spiritually, acknowledge that belief, then ask how the other partner's voice can be equally integrated. Reframe this not as a challenge to doctrine but as a relational agreement needed for both parties to participate fully. In cases reminiscent of the Vance dynamic, where pressure to convert may be implicit, invite the couple to discuss what it means to respect each other's spiritual journey without demands. This validates both the religious spouse's identity and the other's autonomy.
Navigating Children's Religious Identity
The Vances are raising three children in the Christian faith, a decision common in interfaith families but one that can become a flashpoint. MFTs must tread carefully here: children's religious upbringing is a values-laden topic where protective instincts escalate quickly. Help parents explore what rearing means in practice (weekly services? religious education? rites of passage?) and negotiate compromises that acknowledge both traditions without forcing a false equivalence. Often, couples find room for both faiths by emphasizing shared morals and allowing each parent to share their heritage in age-appropriate ways. Practitioners who have pursued a divorce and blended family therapist specialization are particularly well-positioned to guide these negotiations, since interfaith parenting disputes can follow patterns similar to blended-family dynamics. The goal is not to prescribe an outcome but to keep the conversation productive and non-coercive.
Questions to Ask Yourself
When a couple presents with conflicting views on faith in therapy, whose comfort level are you unconsciously defaulting to?
Aligning automatically with the more secular partner can alienate the faith-oriented spouse and signal that therapy devalues religion.
Have you explored your own biases about specific religious traditions, positive or negative, and how they might shape your interventions?
Unexamined favoritism or skepticism toward certain faiths distorts case formulation and can undermine treatment for religious clients.
If a client's faith community contradicts your clinical recommendations, can you articulate your rationale without dismissing their spiritual authority?
Clients often weigh pastoral guidance heavily; honoring their spiritual framework while explaining clinical reasoning preserves the alliance.
Integrating Faith Into MFT Sessions: What the Evidence Shows
The Evidence Base for Faith-Integrated Therapy
A comprehensive 2018 meta-analysis by Captari and colleagues, pooling 97 studies and over 7,000 participants, demonstrated that faith-integrated therapy produces large effect sizes (0.74) for both psychological and spiritual outcomes when compared to no treatment.1 When directly compared to secular therapy, faith-integrated approaches showed a small-to-moderate advantage: a 0.33 effect size for psychological symptoms and 0.43 for spiritual well-being.1 These gains were additive, meaning the faith accommodation offered benefits beyond what evidence-based secular therapy alone provided (psychological additive effect 0.13; spiritual additive 0.34). Reliable improvement rates reached 60% for those receiving faith-adapted care.2 The majority of studies focused on Christian populations, with common presenting issues including depression, anxiety, substance use, and trauma, and the most researched modality was religiously accommodative cognitive behavioral therapy (CBT).1 More recent integrative reviews covering 25 studies from 2019 to 2020 affirm these findings in real-world clinical settings.3
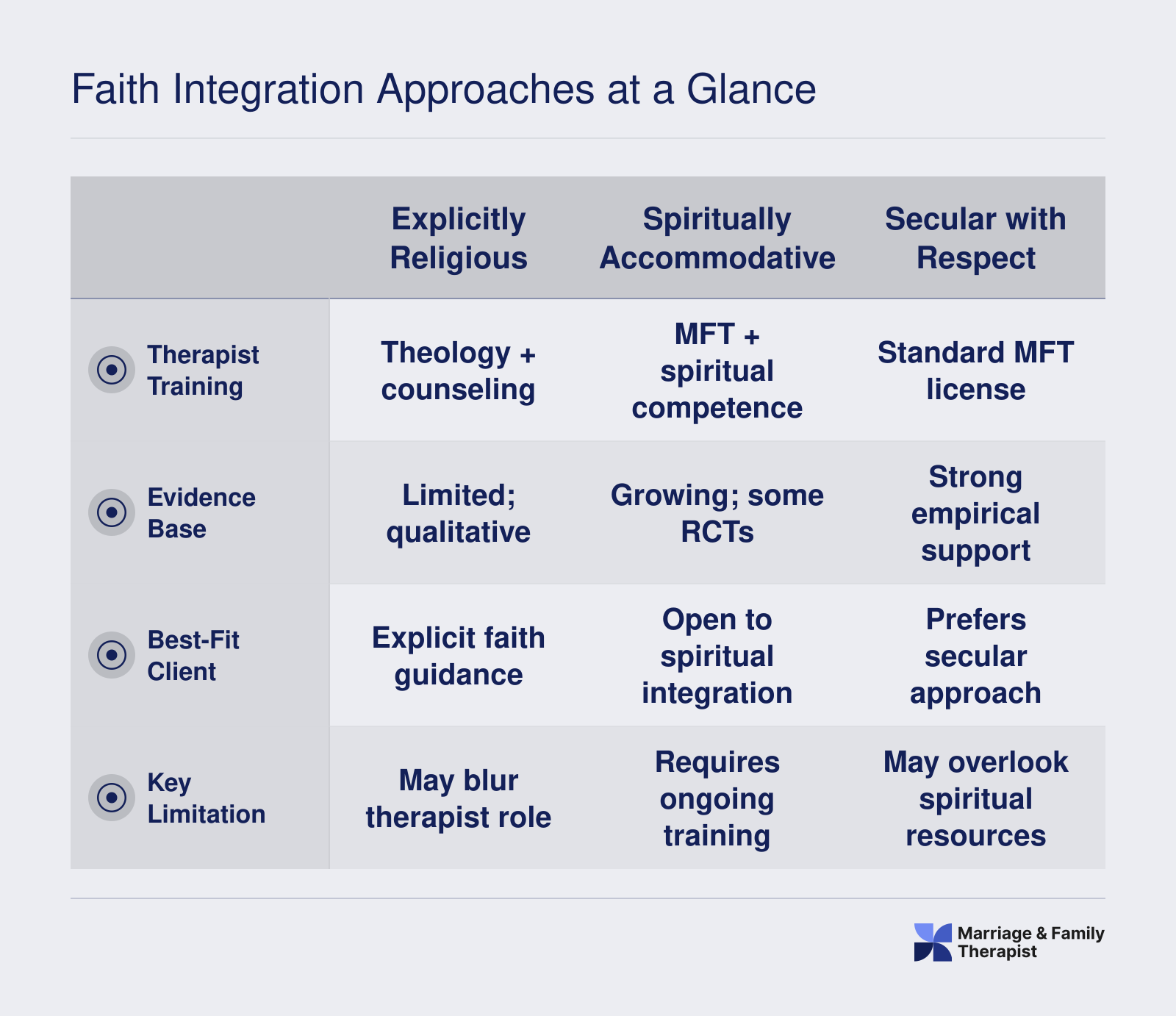
Three Models for Addressing Faith in the Therapy Room
MFTs generally encounter three models when religion enters the clinical space. The first is explicitly religious counseling, where faith provides the overarching interpretive framework and treatment goals (e.g., a Christian counseling center that uses prayer and scripture as primary interventions). The second, spiritually accommodative therapy, integrates a client's personal faith into an evidence-based modality like CBT or emotionally focused therapy, respecting the client's beliefs while still adhering to established therapeutic techniques. The third is secular therapy that politely brackets religion: the therapist acknowledges faith but neither utilizes nor challenges it, focusing entirely on non-religious interventions.
Evidence strongly favors the accommodative model for religious clients. The Captari meta-analysis found that when therapists tailored standard treatments to incorporate clients' religious language and practices, outcomes matched or exceeded those of secular versions, with higher satisfaction and lower dropout.1 Explicitly religious counseling can be effective, but its applicability narrows when working with couples of mixed faiths or those questioning their beliefs.
Faith-Accommodated Approaches in Couples Counseling
The question of whether faith-based and secular therapy can be combined is especially urgent in couples work. The short answer is yes: when both partners consent and the therapist is trained to navigate religious diversity. For couples where one partner prioritizes faith and the other feels skeptical, a spiritually accommodative MFT can integrate the believing partner's language (e.g., referencing biblical concepts of commitment) while maintaining secular interventions like communication skills training. Research on couples therapy specifically shows that accommodating religious values can deepen the therapeutic alliance and reduce resistance, though the therapist must remain vigilant against favoritism or coercion. This integrative stance allows the couple to leverage shared moral frameworks without abandoning clinical rigor.
Faith Integration Approaches at a Glance
Marriage and family therapists can choose from several approaches when incorporating clients' faith into sessions. Each model offers distinct benefits and training requirements, depending on the client's spiritual needs and the therapist's competencies.
When Faith Integration Can Harm: Religious Trauma, Coercion, and Contraindications
Defining Religious Trauma and Spiritual Abuse
The mental health field is sharpening its diagnostic understanding of religious trauma, recognizing that harmful faith experiences produce symptom clusters indistinguishable from other trauma disorders. An estimated 27 to 33 percent of U.S. adults report experiences consistent with religious trauma, a condition marked by PTSD-like symptoms, anxiety, depression, and shame rooted in coercive spiritual environments.1 Spiritual abuse specifically uses religious teachings to manipulate, control, or shame, with common tactics including enforced obedience, public humiliation, and rules that forbid questioning authority.2 For survivors of purity culture, clinical presentations often involve sexual shame, body dissociation, and obsessive religious scrupulosity even in the absence of a discrete assault.1 VA and Department of Defense clinical guidelines note that negative religious coping styles, such as feeling abandoned by God, predict poorer mental health outcomes after trauma.3
Contraindications for Faith Integration
While spiritually integrated therapy benefits many, several circumstances demand caution. First, when a client has unprocessed religious trauma, introducing faith language without explicit informed consent risks retraumatization.1 Second, in couples work, one partner may leverage religious authority to coerce the other; this power dynamic undermines safety and must be addressed before any faith content is incorporated. Third, therapists whose personal convictions would prevent clinical neutrality regarding a client's religious choices should refer out or seek supervision.2 Finally, spiritually directive approaches, where the therapist assumes a pastoral role, are contraindicated outside of explicitly requested and bounded pastoral counseling.
The LGBTQ+ Dimension: Safety First
The highest-risk scenario occurs with LGBTQ+ clients whose faith traditions condemn their identity. Conversion therapy efforts, even when framed as spiritual guidance, consistently elevate risks for depression, anxiety, and suicidality, and are considered unethical and harmful.1 MFTs working in this space benefit from LGBTQ+ affirming therapy training to ensure they can screen for histories of religious rejection or coercive discipleship. A spiritually integrated approach that validates a client's internal conflict while failing to challenge the doctrine labeling them as sinful can retraumatize. Safety overrides accommodation: the client's well-being must take precedence over any request to work within a non-affirming faith framework.
A Decision Framework for MFTs
When a client requests faith integration, begin by exploring their spiritual history: was their religious past primarily supportive or harmful? Screen for trauma-like reactions to religious stimuli, which differentiate ordinary spiritual struggle from religious trauma syndrome.1 In couple or family therapy, evaluate whether one member uses religious authority as a control tactic; if so, faith integration cannot proceed until this dynamic is resolved. Ask whether the client's faith framework supports or undermines their stated therapeutic goals; if the religious system is part of the problem, integration is contraindicated. Collaborate only with faith leaders whom the client experiences as safe, and only with informed consent.2
If a client's religious community has deemed therapy sinful or unnecessary, the therapist confronts more than distrust, spiritual coercion may be operating. The ethical obligation is unequivocally to the client's well-being, never to the community's authority. Prioritize the client's safety and autonomy above all external pressures, and respond with careful advocacy.
How to Find an MFT Trained in Religious and Spiritual Competence
Some clients seek a therapist who shares their exact faith tradition; others prioritize clinical competence in integrating spirituality regardless of denominational match. Both paths require screening beyond self-reported labels.
For Clients: What to Ask Before Scheduling
When contacting a potential MFT, go deeper than a directory checkmark. Inquire about their training with ASERVIC competencies, which cover assessing spiritual beliefs, managing religious countertransference, and designing spiritually accommodative interventions. Ask directly: "How do you typically handle sessions when a client's faith conflicts with therapeutic goals?" Their answer reveals whether they practice spiritually accommodative therapy (adapting standard modalities) or explicitly religious counseling that draws on scripture, prayer, or clergy collaboration. Request examples of how they have worked with clients from your specific faith tradition. A therapist who has never handled a Catholic scrupulosity case or a Muslim couple negotiating gender roles may lack the nuance you need.
For Aspiring MFTs: Training That Builds Spiritual Competence
Graduate programs vary in how deeply they cover religious diversity. CACREP accreditation requires multicultural competence, but coursework on spirituality is often elective. Look for programs offering concentrations or certificates in spiritual integration. Continuing education matters: post-degree workshops through AAMFT or the American Association of Pastoral Counselors can fill gaps. Seek supervision from practitioners experienced in faith-accommodative work, and consider how MFT clinical internship training exposes trainees to diverse client worldviews before licensure. If you want to specialize, pursue credentialing like the Certified Clinical Spiritual Care Provider designation, which signals advanced training in bridging clinical and faith-based perspectives.
Using Therapist Directories Strategically
Psychology Today and TherapyDen let you filter by "Spirituality" or "Christian Counseling," but these are self-reported and rarely verified. A therapist who checks "Christian" may simply feel comfortable with religious clients, not actually integrate faith into sessions. In your consultation call, ask: "What specific training have you completed in religious or spiritual competence?" and "Can you describe your approach when a client's religious beliefs conflict with evidence-based treatments?" These questions expose whether the therapist relies on personal faith or formal training.
Shared Faith vs. Spiritual Cultural Competence
The best-trained MFT for a religious client may not share their denomination. Cultural competence means understanding how faith shapes worldview, family dynamics, and help-seeking behaviors, not necessarily practicing that faith yourself. An MFT with robust training in internal family systems therapy or similar relational modalities can serve a Hindu couple as effectively as a Hindu therapist, provided they avoid proselytizing and honor the client's belief system. What matters is respectful curiosity, ethical boundaries, and the ability to distinguish between clinically appropriate faith integration and coercive religious influence.
Frequently Asked Questions About Faith and Therapy in MFT Practice
The intersection of faith and therapy raises critical questions for marriage and family therapists. Drawing from ethical guidelines, clinical evidence, and real-world cases, the following answers address common concerns about navigating religious skepticism and spiritual integration in MFT practice.
How should a therapist respond when a client prefers faith over therapy?
Therapists should respect the client’s autonomy and worldview. Begin by exploring what makes faith feel more trustworthy or effective than therapy for them. Validate their experience, avoid defensiveness, and clarify that therapy can complement, not replace, spiritual practices. Offer to collaborate with faith leaders if appropriate, while maintaining professional boundaries per AAMFT ethics.
Can faith-based therapy and secular therapy be combined in couples counseling?
Yes, when both partners consent and the therapist is competent to integrate spiritual dimensions. The therapist must assess whether religious beliefs are a source of conflict or a unifying resource. Use a spiritually integrated approach that respects each partner’s perspective, ensuring that no one’s beliefs are imposed. Clear communication and mutual agreement on therapy goals are essential.
What are the AAMFT ethical guidelines on religion and spirituality in therapy?
The AAMFT Code of Ethics requires non-discrimination on the basis of religion and calls for cultural competence, including spiritual awareness. Therapists must avoid imposing their own beliefs, respect clients’ religious values, and practice within their scope of competence. When faith issues arise, therapists should seek consultation or refer if they cannot provide culturally responsive care.
When does integrating faith into therapy do more harm than good?
Faith integration becomes harmful when it coerces, shames, or reinforces religious trauma. It is contraindicated when clients feel pressured to adopt religious solutions, when spiritual bypassing ignores mental health needs, or when faith differences between partners are weaponized. Therapists must continually assess for safety and avoid substituting religion for necessary clinical interventions.
How does religion affect ethical decisions in family therapy?
Religion can shape family hierarchies, gender roles, and views on autonomy, confidentiality, and forgiveness. Ethical decisions require careful attention to how faith influences family dynamics and individual rights. MFTs must balance respect for religious values with the duty to protect vulnerable members and uphold professional ethics, ensuring no harm is done in the name of faith.
What is ethical skepticism in the context of therapy and research ethics?
Ethical skepticism refers to a cautious, questioning approach that prioritizes client welfare over untested claims or personal bias. In therapy, it means critically evaluating the efficacy of faith-based interventions and remaining open to evidence. In research, it involves scrutinizing methods and assumptions to avoid harm, ensuring that spiritual integration is based on sound clinical reasoning.