Key Studies on MFT Effectiveness and Long-Term Client Outcomes
Research on marriage and family therapy (MFT) models reveals a consistent picture: when delivered with fidelity, these approaches produce meaningful, durable change for couples and families. This section synthesizes key follow-up data from major MFT modalities, highlights meta-analytic support, and addresses an important gap in the literature.
The Durability of Emotionally Focused Therapy Gains
Emotionally focused therapy stands out for its strong empirical base. A seminal meta-analysis published in 1999 reported an overall effect size of 1.3, with 70, 73% of couples recovering from relationship distress and roughly 90% showing significant improvement.1 Notably, gains not only held but often increased after therapy ended. Johnson and Greenberg (1985a) documented that recovery rates rose from 46% immediately post-treatment to 73% at follow-up.2 A later trial by Johnson and Talitman (1997) replicated this pattern: 50% recovery at termination climbed to 70% in the subsequent months.2
A closer look at long-term trajectories comes from Cloutier et al. (2002), who tracked couples for up to two years. They found that 23.1% maintained the gains they had made in therapy, while a substantial 38.5% continued to improve on their own.3 An additional 30.8% showed no significant change, and only 7.7% deteriorated. This distribution underscores that EFT often equips couples with lasting relational skills. Walker and Manion (1998) similarly observed that therapeutic improvements were maintained at a two-year follow-up.2
Long-Term Evidence for Functional Family Therapy and the Gottman Method
Functional Family Therapy (FFT) has amassed longitudinal data with adolescents and their families, demonstrating reductions in recidivism and improvements in family functioning that persist for several years. Multiple studies indicate that families completing FFT continue to benefit well beyond the active treatment phase, with follow-up assessments often extending to three or five years. The Gottman method therapy, grounded in decades of observational research on couples, also shows sustained impact. Follow-up studies, while varying in duration, typically find that the majority of couples who initially improved retain enhanced relationship satisfaction and communication patterns.
Systemic Approaches and the AAMFT Evidence Base
The American Association for Marriage and Family Therapy (AAMFT) routinely updates a registry of evidence-based practices. Meta-analyses on systemic family therapy broadly confirm its effectiveness, with stable effects across diverse presenting problems. These aggregated reviews reinforce that MFT models, on average, outperform no-treatment controls and often rival or surpass individual therapies for relational concerns. The evidence is especially strong for conjoint approaches targeting depression, adolescent conduct problems, and marital conflict.
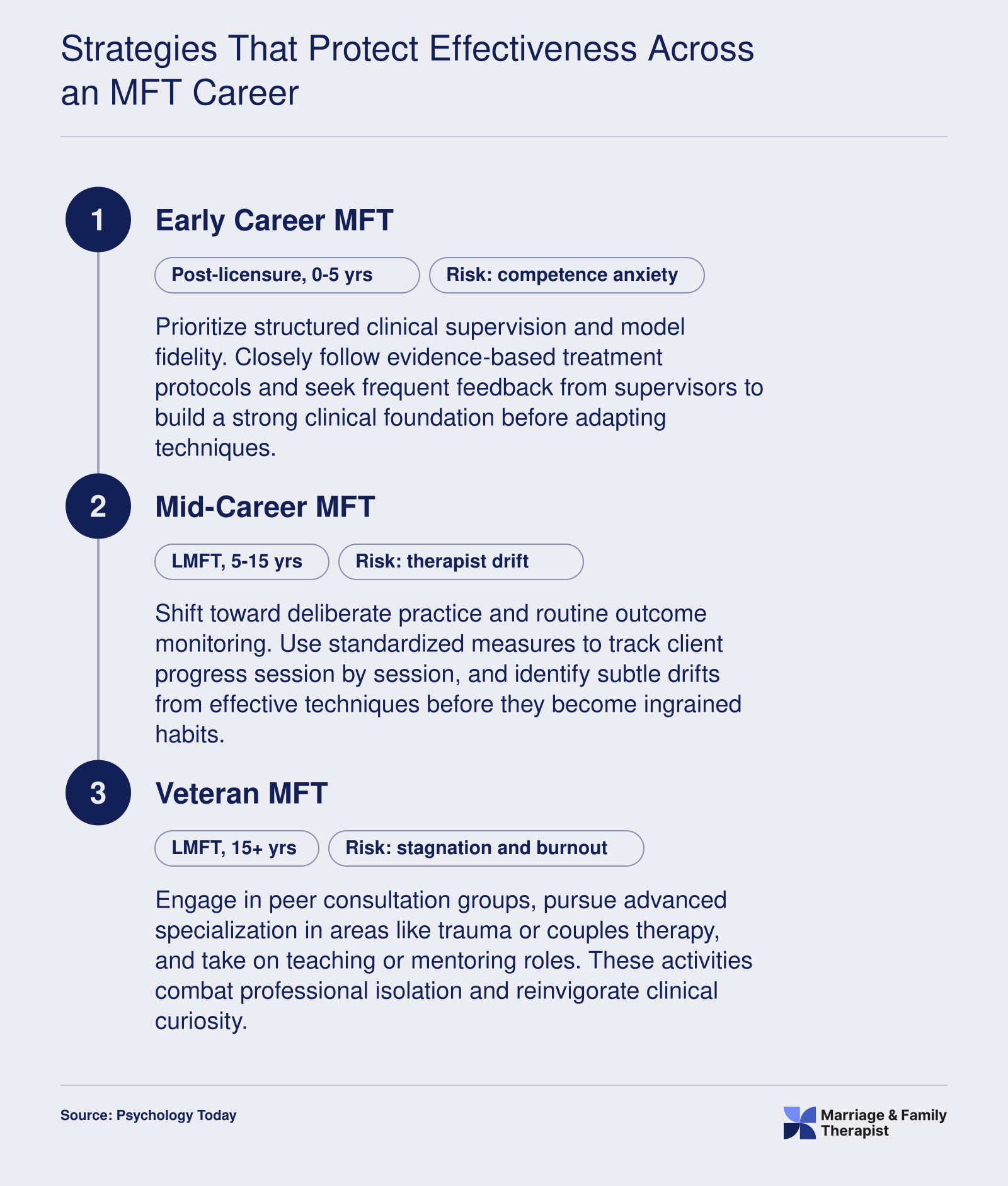
A Critical Distinction: Model Efficacy vs. Therapist Trajectory
It is essential to recognize what these studies do and do not measure. Most long-term outcome research in MFT evaluates whether a specific treatment protocol produces lasting change when administered by trained clinicians under research conditions. They do not track how the outcomes of a single therapist evolve over the course of a decades-long career. The data speak to the therapy's potential, not to the individual provider's sustained skill level. This gap matters because, as discussed earlier, some evidence suggests therapist effectiveness can plateau or decline without deliberate maintenance. Therefore, a therapist who delivered strong results with EFT or FFT early in their career may not achieve the same outcomes years later unless they actively guard against drift and complacency.
The implication is sobering but actionable: the models work, but they deliver their full benefit only when therapists continue to apply them with fidelity. The durability of client gains depends on a practitioner's ongoing commitment to skill refinement, supervision, and feedback, not merely on the passage of time or accumulation of experience.