Narrative Therapy: Techniques, Evidence & MFT Practice
Narrative Therapy: How It Works, Key Techniques & Who It Helps
A comprehensive guide to narrative therapy's core concepts, session structure, evidence base, and how marriage and family therapists apply it in practice.
Michael White and David Epston developed narrative therapy in the 1980s on a postmodern, social constructionist foundation.
Core techniques include externalization, unique outcomes mapping, re-authoring conversations, outsider witness practices, and therapeutic letter writing.
RCTs show positive outcomes for depression, anxiety, PTSD, and family conflict, though the evidence base remains smaller than that of CBT.
Training typically ranges from short workshops costing a few hundred dollars to multi-year certificate programs exceeding 5,000 dollars through institutes like Dulwich Centre.
Developed in the 1980s by Australian social worker Michael White and New Zealand therapist David Epston, narrative therapy is a collaborative, non-pathologizing approach rooted in postmodern and social constructionist theory. It treats clients as the experts of their own lives, not as collections of symptoms waiting to be diagnosed. Problems are separated from people and examined as stories that can be questioned, rewritten, and replaced.
The approach has gained steady traction among marriage and family therapy modalities, yet it lacks a single credentialing body, which means training paths vary widely in cost, depth, and clinical recognition. For MFTs weighing whether to invest in narrative specialization, the absence of a standardized certificate makes informed comparison especially important.
What Is Narrative Therapy? Origins, Philosophy, and Core Model
Narrative therapy is built on a postmodern premise that sets it apart from most mainstream psychotherapy models: the stories people tell about their lives are not neutral reflections of reality but active constructions that shape how they feel, relate, and behave. When a person's dominant story becomes "problem-saturated," meaning it defines them primarily through deficit, failure, or pathology, the therapy's goal is not to correct distorted thinking (as in CBT) or interpret unconscious conflict (as in psychodynamic work). Instead, the clinician helps the client separate themselves from the problem, recover overlooked experiences that contradict the dominant narrative, and ultimately author a richer, more preferred account of who they are. This is not talk therapy rebranded. It is a fundamentally different way of understanding how problems are created and how change happens.
Intellectual Roots: Foucault, Bateson, and Bruner
Michael White and David Epston, the Australian and New Zealand therapists who formalized narrative therapy in the late 1980s and early 1990s, drew on an unusually interdisciplinary set of ideas.
Michel Foucault (power/knowledge): Foucault argued that dominant cultural discourses determine what counts as "normal" and who gets labeled as deviant. White adapted this lens to therapy, encouraging clients to examine how societal norms, diagnostic categories, and family rules had authored their problem stories without their full consent.
Gregory Bateson (cybernetics and ecology of mind): Bateson's systems thinking taught White that meaning never lives inside one person alone; it circulates through relationships and feedback loops. Narrative therapy therefore pays close attention to the relational context in which stories are told and maintained.
Jerome Bruner (narrative psychology): Bruner's research demonstrated that humans organize experience primarily through narrative rather than logic. White and Epston used this insight to argue that reshaping the story is not a metaphor for change; it is the mechanism of change.
This combination of social critique, systems theory, and cognitive science gives narrative therapy a distinctive theoretical identity that practitioners should understand before they pick up its techniques.
The Therapist's Stance: Decentered but Influential
A narrative therapist does not sit back and interpret, nor does the therapist assign homework or teach coping skills in the way a cognitive-behavioral clinician might. The stance is described as "decentered but influential." The clinician remains genuinely curious, asking carefully crafted questions that guide the client toward new meanings, yet never positioning themselves as the expert on the client's life. The client is the author; the therapist is more like a collaborative editor who highlights passages the author overlooked and asks, "What if this chapter matters more than you thought?"
This posture has practical implications. Sessions tend to be heavy on open-ended, exploratory questions and light on directives. The therapist's influence shows up in the choice and sequencing of those questions, not in pronouncements about what the client's experience "really means."
A Versatile Framework Across Settings
Although narrative therapy was initially developed in family therapy contexts, its framework extends well beyond the family consulting room. Clinicians now apply it with individuals, couples, families, groups, and even entire communities (for example, collective narrative practice with refugees or indigenous populations). It is one of several evidence-based family therapy modalities that licensed marriage and family therapists regularly draw from when working across diverse populations and presenting concerns. Later sections of this guide unpack specific applications in detail, but it is worth noting early that the approach's flexibility is one of its greatest strengths. Practitioners interested in the relational roots narrative therapy shares with other models may also benefit from understanding Bowen family systems theory, which similarly emphasizes how meaning circulates through family relationships.
Core Concepts and Techniques: What Happens in a Narrative Therapy Session
Narrative therapy sessions feel less like a clinical assessment and more like a guided conversation. There is no rigid manual or scripted protocol, but there is a recognizable arc: the therapist and client move from naming and mapping a problem, to separating the person from the problem, to uncovering moments when the problem did not dominate, and finally to building a richer, preferred story. Understanding that arc, along with the specific techniques that drive it, gives you a clear picture of what this approach looks like in real time.
The Signature Techniques
Seven core techniques form the backbone of narrative practice. Each one serves a distinct purpose in the overall therapeutic conversation.
Externalization: The defining move of narrative therapy. The therapist uses language that treats the problem as a separate entity rather than a character flaw. Instead of asking "Why are you so anxious?" a narrative therapist might say, "When did Anxiety first show up in your life? What tactics does it use to convince you that you cannot handle things?" This reframe, often summarized as "the problem is the problem, not the person," immediately shifts a client's relationship with their distress.
Re-authoring (re-storying): Once the problem is externalized, therapist and client collaborate to construct an alternative storyline, one in which the client's values, skills, and intentions take center stage rather than the problem's influence.
Unique outcomes: These are exceptions to the dominant problem story, moments when the client resisted or sidestepped the problem's influence even briefly. Identifying them provides the raw material for the preferred narrative.
Deconstruction: Through careful questioning, the therapist helps the client unpack taken-for-granted beliefs, cultural messages, or power dynamics that keep the problem story in place.
Scaffolding questions: Borrowed from educational theory, these are layered questions that move from the concrete ("What happened?") to the reflective ("What does that say about what matters to you?"), helping clients bridge the gap between lived experience and new meaning.
Definitional ceremonies: Drawn from anthropologist Barbara Myerhans's work, these are structured witnessing practices in which a selected audience reflects on the client's preferred story, thickening it through social acknowledgment.
Therapeutic documents: Letters, certificates, or written summaries created by the therapist (sometimes co-authored with the client) that record milestones, unique outcomes, or declarations of the preferred identity. These documents serve as portable reminders of progress between sessions.
What a First Session Typically Looks Like
A first narrative therapy session usually begins with collaborative goal setting. The therapist invites the client to describe the concern that brought them in, using open-ended, respectful inquiry. From there, the work moves through several phases:
Naming the problem in the client's own language, for example calling it "The Fog" or "The Critic" rather than adopting a clinical label prematurely.
Mapping the problem's influence across different life domains: relationships, work, self-image, daily routines.
Beginning to externalize the problem through conversational language shifts.
Searching for exceptions, times the client acted in ways that contradicted the problem story, even in small ways.
This first session sets the tone for the entire course of treatment. Clients often leave feeling that they have been heard without being pathologized, which is one reason narrative therapy builds strong therapeutic alliance quickly.
Externalization in Action: A Brief Dialogue
To make the technique tangible, consider this exchange between a therapist and a client struggling with persistent self-doubt:
Therapist: "You mentioned that Self-Doubt has been running the show at work. When did Self-Doubt first start whispering to you that your ideas were not good enough?"
Client: "Probably around middle school, when a teacher told me my writing was mediocre."
Therapist: "So Self-Doubt has been around for a long time. Are there moments at work when Self-Doubt steps back, even just a crack, and you hear your own voice instead?"
Notice that the therapist never says "you doubt yourself." The language consistently positions the problem outside the person, opening space for curiosity rather than shame.
Session Structure and Typical Course of Treatment
Narrative therapy does not follow a manualized week-by-week protocol. Instead, sessions follow a general progression: problem naming gives way to externalization, which gives way to discovering unique outcomes, which gives way to thickening the preferred story through re-authoring, witnessing, and documentation. The pace depends entirely on the client.
A typical course of treatment ranges from roughly 6 to 20 sessions, though it can be shorter for focused concerns or longer for deeply entrenched narratives. For context, cognitive behavioral therapy protocols for conditions like depression or anxiety generally run 12 to 16 sessions. Narrative therapy's range is comparable but tends to be more flexible because progress is measured by the richness of the emerging story rather than by symptom checklists alone. This flexibility makes it especially appealing to therapists who want to honor each client's unique timeline. Compared with other marriage and family therapy modalities such as structural family therapy or emotionally focused therapy, narrative therapy stands out for the way it centers the client's own language and meaning-making throughout every phase of treatment.
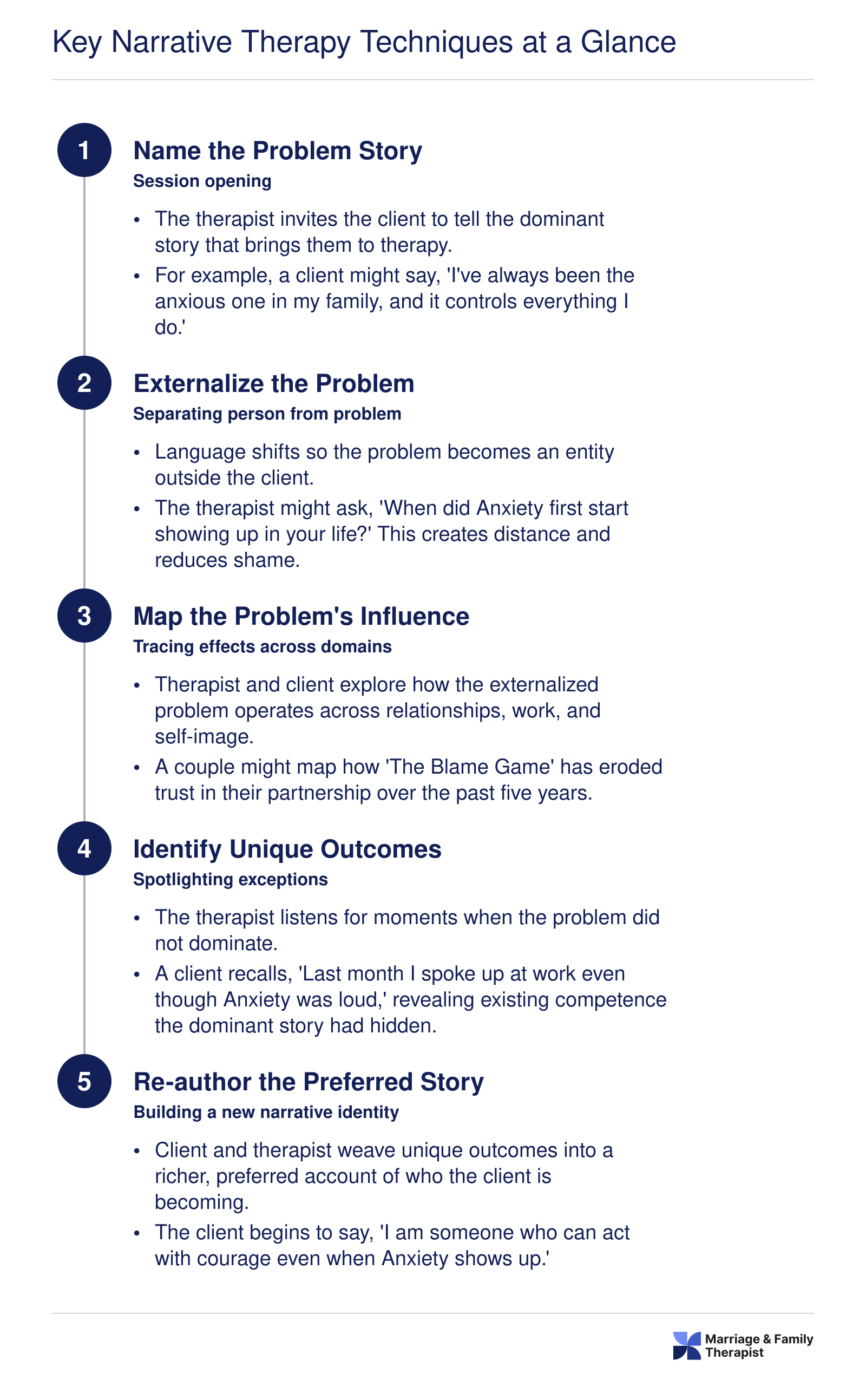
Key Narrative Therapy Techniques at a Glance
Narrative therapy follows a collaborative sequence that helps clients move from problem-saturated stories toward preferred identities. Below is the typical five-step process a therapist guides in session, with a brief clinical example at each stage.
Who Narrative Therapy Helps: Populations, Diagnoses, and Settings
Narrative therapy's emphasis on meaning-making and personal agency gives it unusually broad applicability. Rather than targeting symptoms in isolation, the approach helps clients reauthor the stories that hold those symptoms in place. That flexibility makes it relevant across a wide range of presenting issues, age groups, and cultural contexts.
Presenting Issues With Strong Practice Support
Clinicians report the most consistent results when narrative methods are applied to:
Depression and anxiety: Externalizing "the depression" or "the worry" helps clients see themselves as separate from their distress, reducing shame and opening space for action.
Trauma and PTSD: Re-storying traumatic events lets clients reclaim a sense of authorship over their own lives. This work is often done alongside stabilization techniques from other modalities.
Grief and loss: Narrative practices such as "re-membering" conversations help mourning clients honor their relationship with the deceased while building a forward-looking identity.
Eating disorders: Naming the eating disorder as an external influence (sometimes literally giving it a name) can weaken its grip and clarify the client's own values around nourishment and self-care.
Identity concerns: Individuals navigating LGBTQ+ identity, immigration, or cultural dislocation benefit from examining how dominant cultural narratives have shaped their self-concept, then crafting preferred stories that better reflect their lived experience.
Couples and Family Work
Narrative therapy is a natural fit for relational settings. When a problem is externalized, couples and families can unite against the issue rather than blame each other. A family struggling with conflict, for example, might come to see "the arguing" as a shared adversary. This shift lowers defensiveness and opens collaborative problem-solving. Therapists working with couples often find that narrative questions reveal hidden assumptions each partner carries about roles, loyalty, and love, giving the dyad a shared language for renegotiating those stories.
Children and Adolescents
Younger clients respond especially well to playful externalization. A child dealing with anger might draw "the temper monster" and then brainstorm strategies for keeping it in its cage. Naming the problem as a character transforms therapy from an intimidating adult conversation into an imaginative, empowering exercise. This makes narrative methods popular in school counseling offices and pediatric settings alike. Clinicians interested in this population can explore how to become a child and adolescent therapist for a detailed career roadmap.
Marginalized and Cross-Cultural Populations
Few therapeutic frameworks pay as much explicit attention to power, privilege, and cultural context. Narrative therapy invites clients to interrogate whose stories have been centered and whose have been silenced. For communities affected by racism, colonization, or systemic inequity, this orientation validates lived experience in a way that culturally neutral models may not. Practitioners in community mental health, refugee services, and Indigenous health programs frequently draw on narrative principles for this reason. Clinicians who want to deepen this competency may also pursue LGBTQ+ affirming therapy training to complement narrative skills with identity-specific clinical frameworks.
Integration With Other Modalities
In everyday clinical practice, narrative therapy rarely operates in a vacuum. Many therapists blend narrative techniques with cognitive-behavioral strategies, solution-focused questioning, or attachment-based frameworks like the Gottman method. A clinician might use externalization to soften a client's relationship with anxiety and then introduce CBT-style thought records once the client feels less identified with the problem. This integrative flexibility is one of the approach's greatest practical strengths, allowing it to enhance almost any treatment plan rather than compete with it.
Narrative therapy's externalization technique can be a game changer for couples. Instead of framing a partner as the source of conflict, both people learn to say "the problem is the problem." This simple shift lowers defensiveness almost immediately and opens real space for collaboration, turning adversaries into teammates working against a shared challenge.
Evidence Base and Outcomes Research
Narrative therapy occupies a distinctive space in the clinical research landscape. It is widely recognized as an evidence-informed approach with a growing body of outcome studies, though it has not yet accumulated the volume of large-scale randomized controlled trials (RCTs) that older modalities like cognitive behavioral therapy (CBT) can claim. For aspiring marriage and family therapists weighing which therapeutic tools to invest in, understanding both the strengths and the honest gaps in the evidence is essential.
What the Research Shows
Several published studies and reviews offer encouraging findings across a range of populations and presenting concerns.
Vromans and Schweitzer (2011): This RCT compared narrative therapy to CBT for adults with major depression. The narrative therapy group showed significant reductions in depressive symptoms at post-treatment and follow-up, with outcomes comparable to those in the CBT group. The study provided early evidence that narrative therapy can hold its own against an established gold-standard intervention for depression.
Lopes et al. (2014): A systematic review examined narrative therapy outcomes across multiple presenting problems, including depression, anxiety, and relational distress. The authors concluded that narrative therapy demonstrated positive effects, particularly in qualitative measures of client well-being and identity reconstruction, though they noted that sample sizes were often small.
Etchison and Kleist (2000): An early review of narrative therapy research documented consistent qualitative improvements across case studies and small trials, particularly in family therapy settings. While not a meta-analysis in the traditional sense, this review helped establish narrative therapy's credibility as a clinically meaningful approach.
More recently, a 2024 systematic review published in PubMed Central examined narrative therapy for people with cancer. The review identified nine studies (five RCTs and four quasi-experimental designs) from a broader corpus of 41 publications.1 Among RCTs involving breast cancer patients, sample sizes ranged from 60 to 120 participants. The findings were notable: effect sizes for reductions in fear of cancer recurrence reached as high as negative 2.89, a large effect, while improvements in health-related quality of life and emotional functioning fell in the medium-to-large range (0.5 to 0.8). However, the reviewers flagged high risk of bias across included RCTs and relatively short follow-up periods of one to four months, which tempers how definitively these results can be interpreted.1
Where Narrative Therapy Stands in Practice Guidelines
Narrative therapy is not currently listed as a first-line treatment in major clinical practice guidelines for conditions like depression or PTSD in the way that CBT or EMDR are. In practice, however, clinicians regularly use it as a primary modality for identity-related concerns, grief, and culturally diverse populations where the approach's emphasis on personal meaning-making and social context resonates strongly. Therapists working with Indigenous communities, refugees, and other marginalized groups have documented promising outcomes when narrative methods are adapted to honor collective storytelling traditions.
For anxiety and PTSD, narrative therapy is more often used as a supplementary approach alongside treatments that have deeper RCT support, or it is employed as the primary framework when clients respond poorly to more directive modalities. Clinicians interested in trauma-focused work can explore how to become a trauma therapist for a closer look at the training involved.
Honest Limitations of the Evidence
Several factors explain the relatively modest research base compared to CBT or other manualized therapies.
Narrative therapy is intentionally flexible, collaborative, and responsive to each client's unique story. This makes it difficult to manualize for the kind of tightly controlled research protocols that funding agencies prefer.
Much of the strongest evidence comes from qualitative studies, single-case designs, and small trials rather than large multi-site RCTs.
Follow-up periods in existing studies tend to be short, making it harder to assess long-term durability of treatment gains.
The Dulwich Centre, founded by narrative therapy's co-creators, maintains a curated bibliography of evidence supporting the approach, but independently conducted large-scale trials remain relatively few.2
None of this means narrative therapy lacks clinical value. It means the research infrastructure is still catching up to what practitioners observe in the consulting room. For MFTs evaluating their training investments, narrative therapy offers a well-theorized, culturally responsive framework with a growing, if still emerging, evidence base. Pairing it with a modality that has deeper RCT support (such as EFT therapy for couples or CBT for anxiety disorders) gives clinicians both the relational depth of narrative work and the research backing that insurance panels and clinical supervisors increasingly expect.
Contraindications and Limitations of Narrative Therapy
Like every therapeutic modality, narrative therapy has genuine strengths and real boundaries. Responsible clinicians weigh both when deciding whether to center treatment on this approach or integrate other frameworks. The lists below summarize what narrative therapy does well and where clinical judgment calls for a different or complementary strategy.
Pros
Its non-pathologizing stance helps clients feel respected rather than labeled, encouraging deeper engagement in the therapeutic process.
Cultural sensitivity is built into the model because it treats each person's lived experience and social context as central to meaning-making.
Empowerment focus positions clients as experts on their own lives, fostering agency that extends well beyond the therapy room.
Adaptable across age groups, relationship structures, and presenting concerns, from couples work to community-based family interventions.
Lower risk of re-traumatization compared to exposure-based therapies, because sessions center on re-authoring stories rather than reliving painful events.
The collaborative, curious posture of the therapist makes it accessible to clients who have had negative experiences with more directive treatment models.
Cons
Not recommended during acute psychosis or severe thought disorder, when a client may be unable to engage in coherent storytelling or distinguish narrative from delusion.
Not feasible for clients with significant cognitive impairment that prevents the abstract, language-heavy reflection the approach requires.
Not appropriate as a standalone intervention for active suicidality; crisis stabilization and safety planning must take priority.
Can be counterproductive with narcissistic personality presentations, where externalizing problems may reinforce avoidance of personal accountability.
Considered complementary at best for borderline personality disorder, which typically calls for structured skills training such as DBT.
Too indirect for conditions demanding concrete behavioral protocols, including severe OCD or active substance dependence requiring structured relapse-prevention work.
Not first-line during acute mood episodes or acute trauma, when immediate symptom reduction and stabilization are clinically necessary.
Narrative Therapy Vs. Narrative Exposure Therapy: Key Differences
The shared word "narrative" leads many clinicians and prospective clients to conflate these two modalities, but they are entirely different approaches with distinct founders, goals, session structures, and evidence bases. If you are researching therapeutic options, understanding the distinction is essential.
Origins and Theoretical Foundations
Narrative therapy emerged in the 1980s and early 1990s through the work of Michael White and David Epston. It is grounded in social constructionism and post-structuralism, holding that problems arise from dominant cultural discourses and that healing happens when people re-author preferred life stories.1
Narrative Exposure Therapy (NET) was developed in the early 2000s by Maggie Schauer, Frank Neuner, and Thomas Elbert.2 NET draws on the dual representation model of traumatic memory, using imaginal exposure and chronological contextualization to integrate fragmented "hot" sensory memories with "cold" autobiographical facts.3 It is, at its core, a trauma exposure protocol, not a general orientation to therapy.
Session Format and Structure
The differences in clinical practice are stark:
Narrative therapy: Non-manualized and flexible, typically delivered in weekly sessions of 45 to 60 minutes over a variable number of meetings. The therapist and client collaboratively set the agenda.
NET: Manualized and short-term, structured across 4 to 12 sessions of roughly 90 minutes each. The client constructs a chronological lifeline and narrates each traumatic event in sequence, allowing habituation and cognitive integration.3
Target Populations
Narrative therapy is broadly trans-diagnostic. Clinicians apply it to depression, anxiety, psychosis, relationship conflict, grief, and identity concerns across individuals, couples, and families.
NET is designed specifically for PTSD arising from multiple or chronic traumatic exposures. It has been studied extensively with refugees, survivors of organized violence, and child soldiers, and it is well suited to low-resource settings where long-term therapy is unavailable.2
Evidence Base
NET is backed by multiple randomized controlled trials showing medium to large effect sizes for PTSD symptom reduction.1 It is recommended by the APA as a frontline treatment for trauma-spectrum disorders, and it also appears in guidelines from the World Health Organization and NICE.3
Narrative therapy's evidence base relies more heavily on qualitative studies and case reports, with fewer rigorous RCTs. It is not listed as a first-line intervention in major PTSD treatment guidelines, though it demonstrates promise in broader mental health contexts.
A Simple Decision Heuristic
If you are searching for a structured, evidence-based protocol to treat PTSD, particularly PTSD stemming from repeated or organized trauma, NET is the modality you want. If you are looking for a collaborative, non-pathologizing therapeutic orientation that addresses identity, meaning-making, and a wide range of presenting concerns, narrative therapy is the match. Both approaches are part of the broader landscape of therapy approaches used by MFTs, and the two can even complement each other within a treatment plan, but they should never be confused as interchangeable.
Questions to Ask Yourself
Do you prefer collaborative, non-directive therapeutic relationships over structured, clinician-led interventions?
Narrative therapy positions the client as the expert on their own life. If you thrive when sharing power in the room rather than prescribing homework or protocols, this orientation aligns with your instincts.
Are you more energized by exploring clients' stories than by targeting specific symptoms with measurable scales?
This approach prioritizes meaning-making and identity over symptom reduction checklists. Clinicians who find diagnostic categories too narrow often feel at home here, but those who want manualized structure may not.
Would your ideal caseload benefit from an approach that centers cultural context and power dynamics?
Narrative therapy was built to address how dominant cultural narratives shape personal identity. If you plan to work with marginalized communities, immigrants, or populations affected by systemic oppression, this framework offers tools other models lack.
Are you prepared to invest in ongoing consultation and reflective practice rather than a single certification exam?
Unlike some modalities with clear credentialing endpoints, narrative therapy training is iterative. It requires sustained reading, peer consultation, and self-reflection, so consider whether that open-ended commitment fits your professional development style.
Training and Certification Pathway for Narrative Therapists
Unlike some therapeutic modalities that have a single governing body or standardized credential, narrative therapy does not have one formal certification or accreditation organization. Instead, training is offered through a network of specialized institutes, university programs, and professional workshops. Credentials in narrative therapy are typically certificates of completion issued by the training provider rather than a centralized license or board certification. That distinction matters: before investing time and money, verify that your state or provincial licensing board recognizes the training hours you plan to complete toward continuing education or specialty practice requirements.
Leading Institute-Based Training Programs
Several well-established organizations offer structured narrative therapy education, each with its own format and depth.
Dulwich Centre (Adelaide, Australia): Founded by Michael White, Dulwich Centre is widely regarded as the birthplace of narrative therapy training. The centre offers short workshops, intensive courses, and longer certificate programs delivered both in person and online. Check the Dulwich Centre website directly for current workshop lengths, certificate timelines, and tuition, as these details are updated regularly.
Evanston Family Therapy Center (Evanston, Illinois, USA): This center provides workshops, consultation groups, and extended training sequences rooted in narrative and collaborative practices. Program lengths and fees vary by offering, so consult their course pages for the latest schedule.
Narrative Practices Adelaide: An independent training organization that offers focused coursework in narrative approaches, often in collaboration with practitioners from the broader Adelaide narrative community. Visit their site for current program structures and enrollment information.
Because offerings, costs, and formats shift from year to year, the most reliable step you can take is to research each provider's website directly rather than relying on secondhand summaries.
University-Based Programs
A growing number of universities incorporate narrative therapy into graduate-level training, particularly within marriage and family therapy, social work, and counseling psychology departments. Some institutions offer a dedicated graduate certificate in narrative therapy or narrative practices. To find these, search university program directories for terms like "narrative therapy certificate" or "graduate certificate in narrative therapy." The University of Melbourne, for example, has historically offered coursework connected to narrative approaches, though availability and structure can change. University-based programs tend to carry higher tuition but may count more seamlessly toward graduate degree credit and licensing requirements.
Professional Associations and Standards
While no single body accredits narrative therapists, professional associations can help you evaluate training quality and relevance.
American Association for Marriage and Family Therapy (AAMFT): AAMFT maintains resources on recognized continuing education providers and can help you determine whether a given program's hours satisfy your licensure renewal requirements.
International Society for Ethical Psychology and Psychiatry (ISEPP): ISEPP supports practitioners who integrate critical and narrative perspectives into mental health work and may list relevant training opportunities.
Consulting these organizations before enrolling ensures you are not paying for a certificate that your licensing board will not honor.
Costs and Time Investment
Training expenses range widely depending on the provider and format. A single weekend workshop might cost a few hundred dollars, while an extended certificate sequence spanning several months can run into the low thousands. University graduate certificates carry tuition rates consistent with graduate coursework at that institution. Because fees are updated frequently, always confirm pricing on the provider's own website. Budget for travel if you plan to attend in-person intensives, especially those held in Adelaide or other international locations.
Practical Recommendations
If you are an aspiring or early-career marriage and family therapist considering narrative therapy as a clinical specialty, a practical path looks like this:
Start with an introductory workshop from Dulwich Centre or a comparable provider to confirm the approach resonates with your clinical style.
Pursue a longer certificate program or university-based coursework once you are committed.
Seek peer consultation or supervision with a practitioner experienced in narrative methods to deepen applied skill.
Confirm with your licensing board that your chosen training counts toward continuing education or supervision hours.
Narrative therapy is just one of many clinical orientations you can pursue. If you want to compare it with other options, our overview of therapy approaches used by MFTs can help you weigh the alternatives. For therapists drawn to related specialty tracks, learning how to specialize in family systems therapy provides a useful parallel pathway. marriagefamilytherapist.org can help you map this training alongside your broader licensure requirements, so the journey from initial curiosity to competent narrative practice is as clear and efficient as possible.
Narrative Therapy Training at a Glance
There is no single credentialing body for narrative therapy, so training options range from short introductory workshops to full master's degrees. Below are representative figures drawn primarily from Dulwich Centre, the field's foundational training organization.
How Mfts Use Narrative Therapy in Practice
Marriage and family therapists are uniquely positioned to apply narrative therapy because the approach already treats problems as relational rather than individual. In day-to-day clinical work, narrative concepts show up across every major MFT specialty, and most practitioners weave them into an eclectic toolkit rather than practicing narrative therapy as a standalone modality. That flexibility makes the approach a genuine career advantage: it pairs naturally with structural, solution-focused, and emotionally focused frameworks without creating theoretical conflict.
Couples Therapy: Externalizing Blame Cycles
When partners arrive in crisis, each person typically sees the other as the problem. Narrative externalization shifts the target. Consider a couple locked in emotional withdrawal. The therapist invites both partners to name the pattern itself, something like "The Distance." Once The Distance becomes a shared adversary, blame softens and collaboration rises. The couple can explore questions such as, "When did The Distance first show up?" and "What moments have the two of you had where The Distance lost its grip?" This reframing aligns well with the relational systems lens MFTs already bring to couples work.
Family Therapy: Re-Authoring Family Identity
Families often develop a fixed story about who they are, especially after a member's struggle with addiction or mental illness. A narrative-oriented MFT might guide a family through re-authoring after a teenager's substance-use recovery. Instead of the family defining itself around the crisis ("We're the family that almost fell apart"), the therapist helps each member surface overlooked strengths and turning points. The new story might center on resilience, loyalty, or collective problem-solving, giving the family a shared identity that supports ongoing recovery rather than reinforcing shame.
Child and Adolescent Work
Younger clients respond especially well to playful externalization. A child dealing with anxiety might draw "The Worry Monster" and then describe times they outsmarted it. This technique lowers defensiveness, makes abstract feelings concrete, and gives parents a shared vocabulary for supporting their child between sessions.
Addiction Counseling
Separating the person from the substance-use story is central to narrative work in addiction settings. Rather than framing a client as "an addict," the therapist helps them explore how the substance narrative took hold and identify chapters of their life where different values were guiding their choices. This distinction reduces internalized stigma and supports motivation for change. Clinicians interested in this specialty can review addiction therapist licensure requirements for guidance on dual credentialing.
An Eclectic Career Advantage
Relatively few MFTs identify exclusively as narrative therapists. Most integrate narrative techniques (externalization, re-authoring, unique-outcome questions) into a broader practice that may also include cognitive-behavioral, systemic, or emotion-focused methods. Employers and clients alike value this adaptability. Whether you are drawn to couples counseling, family systems work, or addiction treatment, narrative skills enrich your clinical repertoire and strengthen your professional profile. Explore detailed guides on MFT career paths and current salary benchmarks to plan your next step.
Frequently Asked Questions About Narrative Therapy
Whether you are exploring narrative therapy as a potential client or considering it as a clinical specialty, these answers cover the questions practitioners and prospective clients ask most often. For a broader look at therapeutic modalities, visit the therapy approaches resource page on marriagefamilytherapist.org.
What are the main techniques used in narrative therapy?
The signature techniques include externalization (separating the person from the problem), deconstruction of dominant stories, re-authoring preferred narratives, and the use of therapeutic documents such as letters or certificates. Therapists also employ definitional ceremonies and outsider witness practices, inviting trusted people to reflect on a client's emerging story of strength and resilience.
How many sessions does narrative therapy usually take?
There is no fixed protocol length, but many structured research trials have used approximately eight sessions. In clinical practice the number varies widely depending on presenting concerns, client goals, and whether narrative work is the sole modality or part of a broader treatment plan. Some clients benefit in as few as six sessions; others engage in longer courses of care.
Can narrative therapy help with anxiety, depression, or trauma?
Research supports its use for depression in particular: one trial reported that roughly 74 percent of participants showed reliable improvement and about 53 percent met criteria for clinical recovery after eight sessions. Clinicians also apply it to anxiety and trauma, though the evidence base for those concerns is still developing and results should be interpreted cautiously.
Is narrative therapy effective for children and adolescents?
Many practitioners find narrative therapy well suited to younger clients because storytelling, drawing, and play align naturally with how children communicate. It has been used with children experiencing grief, behavioral difficulties, and family transitions. While published outcome studies specifically focused on youth are more limited than those for adults, clinical reports are generally favorable.
How is narrative therapy different from CBT?
Cognitive behavioral therapy (CBT) focuses on identifying and restructuring distorted thought patterns through structured exercises and homework. Narrative therapy, by contrast, centers on the stories clients tell about their lives, exploring how cultural and relational contexts shape those stories. CBT tends to be more directive and symptom focused, while narrative therapy is more collaborative and meaning focused.
Do I need special certification to practice narrative therapy as an MFT?
No separate license is required. Any licensed marriage and family therapist can integrate narrative techniques into practice. However, specialized training through workshops, certificate programs, or supervision with an experienced narrative therapist strengthens competence and credibility. Organizations such as the Dulwich Centre offer recognized training, and many MFT programs include narrative coursework.
Can narrative therapy be used alongside medication or other therapies?
Yes. Narrative therapy pairs well with pharmacotherapy and other modalities. Clinicians often combine it with elements of solution focused therapy, expressive arts, or family systems work. When a client is taking medication for depression or anxiety, narrative therapy can complement that treatment by addressing the meaning and identity dimensions that medication alone does not target.