Cultural Responsiveness, LGBTQ+ Families, and Diverse Family Structures
Black birthing people experience postpartum depression at rates 1.5 to 2 times higher than white populations, yet remain significantly underdiagnosed and undertreated due to provider bias, medical mistrust rooted in historical trauma, and structural barriers to care. Marriage and family therapists working in perinatal mental health must recognize that postpartum depression does not present uniformly across cultures, identities, or family structures. Tailoring assessment, treatment, and engagement strategies to reflect the lived experiences of diverse families is not an add-on skill; it is a core clinical competency.
Cultural Variations in Postpartum Depression Presentation and Help-Seeking
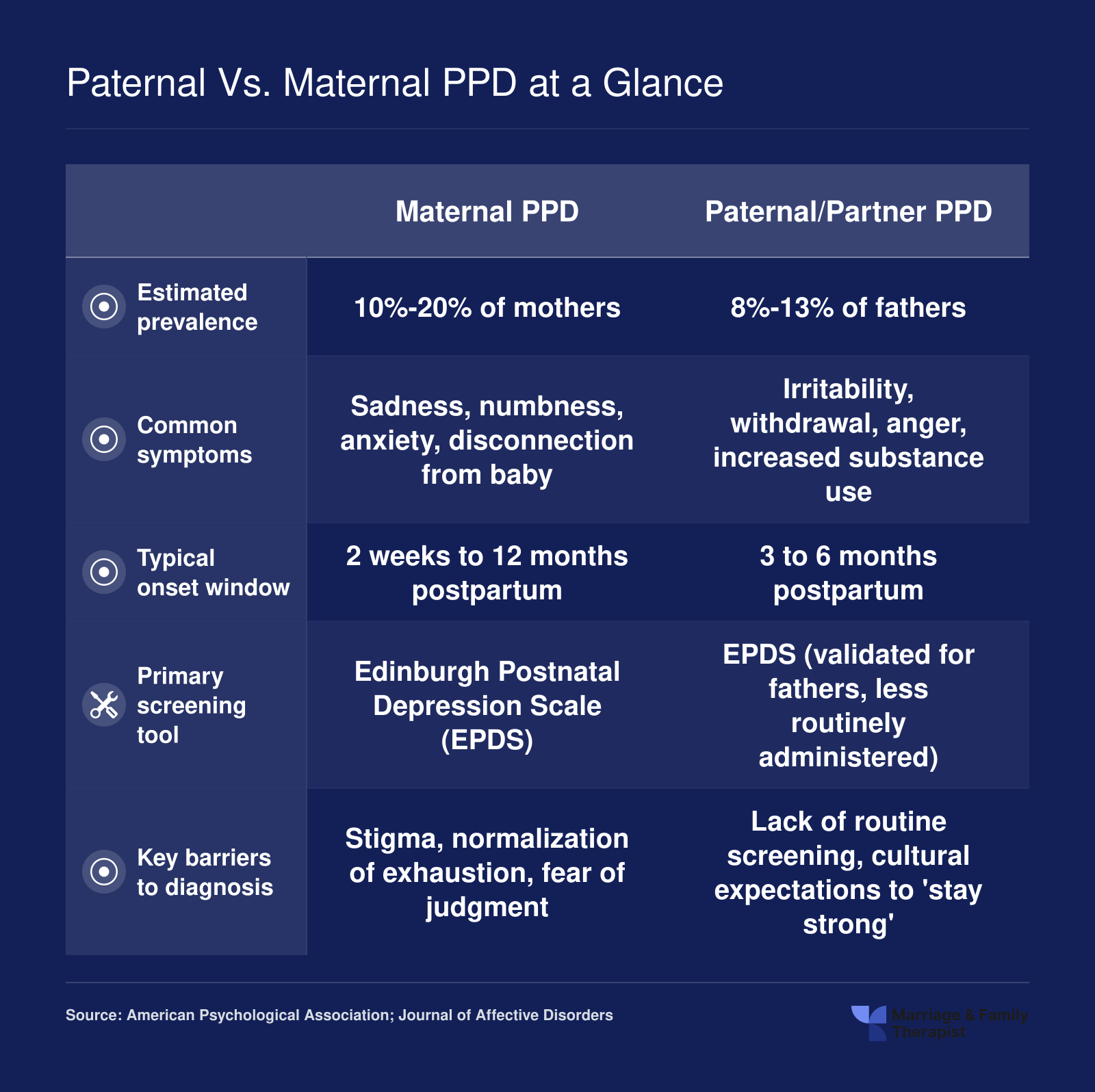
Symptom expression varies by culture. Latinas may describe postpartum depression through somatic language such as nervios or susto, while Asian and Pacific Islander mothers may present with physical complaints (headaches, fatigue) rather than naming sadness or depression directly. Many cultures lack a direct linguistic equivalent for depression, making Western screening tools less reliable. MFTs should use culturally validated instruments when available (for example, the Edinburgh Postnatal Depression Scale has been validated in multiple languages but not all) and supplement standardized scales with open-ended questions about how the client understands distress in their own terms.
Stigma around mental illness is amplified in many communities of color, immigrant families, and faith-centered households. For some clients, admitting difficulty after birth contradicts cultural narratives of motherhood as inherently joyous or sacrificial. Others fear that disclosing postpartum depression will confirm stereotypes or invite child welfare involvement. MFTs should normalize conversations about postpartum adjustment early and often, and acknowledge systemic reasons for mistrust without minimizing client concerns.
Postpartum Depression in LGBTQ+ Couples and Non-Traditional Family Structures
LGBTQ+ parents are largely invisible in postpartum depression research and clinical guidelines, yet they face unique stressors. Non-birthing partners in same-sex couples can develop postpartum depression at rates comparable to birthing parents, particularly when they experience role ambiguity, minority stress, or exclusion from medical appointments and bonding rituals. Adoptive parents and those who used surrogacy also report perinatal mood symptoms but are rarely screened because they did not physically give birth. Clinicians seeking a deeper grounding in LGBTQ+ affirming mental health care will find that affirming frameworks translate directly into more effective postpartum screening for these families.
MFTs must explicitly ask non-birthing partners about mood changes, sleep disruption, and feelings of inadequacy during intake and follow-up. Treatment planning should validate all caregivers as equally central to the family system and avoid gendered language or assumptions about who is struggling.
Concrete Clinical Adjustments for Cultural Responsiveness
MFTs can improve cultural fit through three practical shifts. First, inquire about culturally specific postpartum practices during assessment: confinement periods, dietary restrictions, extended family roles, and spiritual rituals. These practices can be protective or isolating depending on context, and therapists should explore how they are experienced rather than assume universally positive or negative effects. Second, involve culturally significant family members in treatment planning when appropriate. In many cultures, grandmothers, aunts, or elders hold decision-making authority or provide primary childcare support. Excluding them from therapy may reduce intervention effectiveness. Third, screen non-birthing LGBTQ+ partners explicitly for postpartum depression using the same tools and language offered to birthing parents. A single yes-or-no question about gender identity or family formation at intake signals that the practice is affirming and knowledgeable.