Structural, Bowenian, and CBT models each target distinct boomerang family dynamics.
Nearly 60 million U.S. residents lived in multigenerational households in 2021.
Written household contracts and move-out timelines prevent enabling patterns.
More than half of adults 18 to 34 now live in a parent's household, making the boomerang family a presenting issue MFTs encounter weekly. A column by Jim Daly, president of Focus on the Family, published in July 2026, brought this clinical reality into public view: a 23-year-old returning after college, parents unsure how to set rules, and younger siblings watching.1 The advice to treat the son as an adult boarder, with financial contributions and clear boundaries, reads like a lay summary of structural family therapy techniques.
Without a clinical framework that spans assessment, model selection, session contracting, and cultural variation, MFTs risk reinforcing the very patterns families hope to change.
Why Adult Children Are Moving Back Home: Trends MFTs Should Understand
Anecdotal reports from the therapy room versus population-level data: understanding why adult children return home begins with the distinction between what families tell us and what large-scale trends reveal. While every family's story is unique, MFTs are better equipped to normalize, assess, and intervene when they ground clinical impressions in current demographic and economic context. The sources below help therapists move beyond "we never expected him to come back" toward a systemic understanding of multigenerational living.
Finding Demographic Benchmarks
The Pew Research Center makes its detailed survey tables freely available through its online data tools, offering breakdowns of adults aged 18, 34 living with parents by race, gender, and educational attainment. Similarly, the U.S. Census Bureau's Current Population Survey provides annual household composition statistics that can be filtered by region, age, and family structure. Consulting these sources before a first session allows an MFT to say, for example, "You are part of a growing pattern," and to tailor questions around culturally normative versus individually stressful aspects of coresidence. Checking for the most recent year's estimates is essential; proportions can shift within a single economic cycle.
Economic Drivers: Employment, Debt, and Housing
Beyond demographics, the "why" often traces to concrete economic pressures. The Bureau of Labor Statistics (BLS) publishes regular reports on youth employment rates, labor force participation for 20- to 29-year-olds, and median wages by education level, all of which help explain whether a return home reflects a soft job market or a transitional period after graduation. Federal Reserve surveys on student loan balances and housing affordability add another layer: when debt-to-income ratios climb and rental costs outpace entry-level wages, even well-employed young adults may choose to save by living with parents. MFTs can integrate these realities into treatment planning by validating financial stress as a legitimate systemic force rather than a character flaw.
Professional Literature and Specialized Research
Clinical associations and academic centers often compile applied research on boomerang family dynamics. The American Association for Marriage and Family Therapy (AAMFT) and the American Counseling Association (ACA) publish journals and practice briefs linking economic stressors to relational patterns such as parent-child role confusion or delayed differentiation. University research centers studying family resilience or intergenerational relationships may house white papers or data snapshots accessible to practitioners. Modern family therapy guides for MFTs can also bridge the gap between macro trends and micro interventions, offering a foundation for clinical discussions about equity, fairness, and boundary renegotiation inside the home. While population statistics set the backdrop, this professional literature connects systemic context to the practical work MFTs do every day.
Common Relational Patterns and Conflicts in Boomerang Families
The return of an adult child disrupts every relational subsystem in the household, and the disruption follows predictable patterns that MFTs can identify early in treatment.
Role Regression and Structural Hierarchy Disruption
When a 23-year-old moves back into the bedroom they occupied at 16, both parties tend to slip into outdated roles. The adult child may leave dishes in the sink, defer routine decisions to a parent, or revert to a passive stance around household logistics. Parents, in turn, find themselves monitoring curfews, managing meals, and issuing reminders that belong in a parent-teenager dynamic, not a relationship between adults. A July 2026 column in the Crescent-News by Jim Daly, president of Focus on the Family, captures the corrective well: Daly advises parents to treat a returning adult son as "an adult boarder" with clear expectations around order, privacy, and mutual respect.1 From a structural family therapy perspective, this advice targets exactly the right lever. When the family fails to reorganize its hierarchy to reflect the child's adult status, the entire system reverts to an earlier developmental stage, stalling the individuation process for the returning child and trapping parents in a supervisory role they had already outgrown.
Impact on the Parental Partnership
Couples who had begun to reclaim the intimacy and autonomy of an empty nest often experience a jarring reset. Disagreements about how much financial help to offer, how long the arrangement should last, or what rules apply become a new fault line in the marriage. One partner may advocate firm timelines while the other prioritizes emotional support, and the resulting tension can erode the couple subsystem. Spatial boundaries collapse as well: a shared hallway, a thin wall, or the simple awareness that a young adult is home on a Saturday evening can significantly reduce sexual intimacy and spontaneous connection. MFTs should assess the couple relationship early, because unaddressed resentment here radiates outward into every other family interaction.
The Younger Sibling Dynamic
The Daly column describes a household that includes two younger teenagers alongside the returning 23-year-old, and this configuration introduces a particularly destabilizing dynamic. When the older sibling appears to live by a different set of rules (staying out later, skipping chores, or contributing inconsistently to shared expenses) younger siblings perceive the arrangement as unfair, even if the distinctions reflect a legitimate difference in developmental status. Setting boundaries in family therapy is precisely what Daly and Dr. Danny Huerta emphasize: clarifying the distinction between minors and adults in the home is essential for good clinical reason.1 Without that clarity, the sibling subsystem becomes a breeding ground for resentment, boundary testing, and coalitions that undermine parental authority over the teenagers who still need it.
Financial Resentment Patterns
Money is often the loudest flashpoint. Parents who subsidize rent, groceries, car insurance, or student loan payments for the returning child may do so willingly at first, only to feel exploited months later. The adult child, meanwhile, can feel infantilized when a parent attaches conditions to financial support or scrutinizes spending. Daly recommends a financial contribution from the adult child "if appropriate,"1 and that qualifier matters clinically. MFTs should explore whether financial arrangements in the family reflect genuine support or have crossed into enabling dependency. Younger siblings add another layer: a teenager saving money from a part-time job may resent watching an older sibling receive free room and board. These perceptions of inequity, whether accurate or not, corrode trust across the entire family system and deserve direct attention in session.
Questions to Ask Yourself
When a boomerang family presents, do you default to individual work with the adult child, or do you assess the entire family system first?
Individual therapy may miss the relational patterns that sustain dependency or conflict. A systemic assessment reveals how family roles, communication rules, and boundary ambiguity maintain the presenting problem across all members.
Have you examined your own assumptions about what launching should look like, and how those assumptions may differ from your client family's cultural context?
Western norms of early independence do not align with collectivist values common in Asian, Latinx, and many immigrant families. Imposing a timeline rooted in your own worldview can pathologize adaptive, culturally normative arrangements.
Are you assessing the adult child's autonomy or the parents' ability to tolerate differentiation?
Boomerang situations often reflect unresolved separation anxiety in parents as much as immaturity in the child. Treatment goals shift when you identify which subsystem most resists the next developmental stage.
Clinical Assessment: When Is Moving Home Adaptive Vs. Enabling?
The five-item Family APGAR, which screens Adaptability, Partnership, Growth, Affection, and Resolve in a single sitting, offers MFTs a rapid baseline for gauging whether a boomerang household is functioning with mutual respect or fracturing under unspoken resentment.1 Yet no single screening tool replaces the clinical judgment a therapist must exercise in the first session. What follows is a decision framework that helps you distinguish adaptive interdependence from enabling dependence before you ever assign homework.
A Clinical Decision Framework
Three variables should guide your initial assessment when an adult child has returned to the parental home.
First, determine whether the return is time-limited and plan-driven. An adult child who moved home after college graduation with a stated six-month window and an active job search is navigating a life-cycle transition. An adult child who returned "for a while" eighteen months ago with no employment trajectory is a different clinical picture.
Second, evaluate whether the adult child is making measurable progress toward autonomy. That progress can take several forms: holding or actively seeking employment, contributing financially to the household, pursuing education, or building savings. The Comprehensive Family Assessment Guidelines published by the Administration for Children and Families recommend evaluating domains such as life skills, social interaction, and basic necessities.2 These domains translate directly to the boomerang context.
Third, screen for substance use or mental health conditions as the primary driver of the return. When addiction, untreated depression, or anxiety disorders precipitated the move, the treatment plan looks fundamentally different from a financially motivated return. Maladaptive coping strategies are positively correlated with psychopathology, while adaptive coping is associated with improved well-being, according to a review published in PubMed Central.3 Identifying which pattern dominates in the household shapes your entire intervention. MFTs who work with couples addiction therapy will recognize this triage logic from their substance-use casework.
Adaptive Interdependence vs. Enabling Dependence
Adaptive interdependence shows up as mutual benefit, clearly articulated expectations, and cultural congruence with multigenerational living. Both generations contribute something tangible, whether labor, finances, childcare, or emotional support. The arrangement honors each person's developmental trajectory.
Enabling dependence looks different. Parents over-function by managing the adult child's schedule, finances, or social obligations. The adult child under-functions by avoiding developmental tasks such as career planning, cooking, or budgeting. A value-driven negotiation framework developed at the University of Michigan recommends that families establish ground rules rooted in respect and honesty, with regular review periods built in.4 When those ground rules do not exist, enabling tends to fill the vacuum.
Intake Questions That Cut to the Core
MFTs can use the following questions during intake to begin sorting adaptive from maladaptive arrangements:
"What was the stated reason and timeline for your return home, and has that timeline changed?"
"Who initiated the living arrangement, and did the other family members agree or acquiesce?"
"What has changed in the family's daily routines, division of responsibilities, and social lives since the return?"
"How does each family member describe what the adult child is working toward right now?"
These questions surface discrepancies quickly. When the adult child says the plan is "to save money for six months" and the parent says "he just needed somewhere to go," you have already identified a misalignment worth exploring in session.
Differentiation of Self as a Theoretical Lens
Bowen family systems theory provides the theoretical backbone for this assessment through its concept of differentiation of self. A well-differentiated adult child can live under a parent's roof without regressing into adolescent relational patterns. A well-differentiated parent can provide support without reactivating caretaking behaviors that belong to an earlier family life-cycle stage.
When differentiation is low, emotional fusion increases. Parents may monitor the adult child's comings and goings as though managing a teenager. The adult child may respond with passive withdrawal or explosive conflict, recycling patterns the family believed it had outgrown. Using the Conflict Behavior Questionnaire during assessment can help quantify the degree of conflict each party perceives, giving you data to share in session rather than relying on subjective reports alone.1
The goal of your initial assessment is not to label the arrangement as "good" or "bad." It is to determine whether the current structure supports each family member's individuation or quietly undermines it, and then to build a treatment plan that tips the balance toward growth.
Adaptive Vs. Enabling: Key Assessment Indicators
Distinguishing adaptive from enabling dynamics is a core clinical task when an adult child returns home. Without clear indicators, therapists risk endorsing arrangements that erode autonomy or, conversely, pathologizing culturally normative support. The assessment below organizes critical signals across relationship, financial, and developmental domains.
Relational signals of adaptation vs. stagnation
Reciprocity: In adaptive scenarios, the adult child contributes labor, rent, or caregiving. Enabling patterns feature one directional dependency with little documented contribution.
Boundary clarity: Adaptive households renegotiate rules for privacy, guests, and household chores. Enabling homes retain childhood rules or oscillate between overcontrol and permissiveness.
Conflict pattern: Productive tension around roles signals renegotiation; chronic parental rescue from natural consequences of adult choices suggests enabling.
Financial indicators of healthy support
Structured contributions: Adaptive arrangements include a written agreement with a move-out date or savings target. Enabling situations lack any financial plan, and parents absorb costs without clear limits.
Employment trajectory: Adaptive returns coincide with a job search plan, further education, or a startup incubation period. Enabling returns show no consistent employment effort or repeated job losses attributed to external factors.
Developmental markers of differentiation
Emotional autonomy: The adult child maintains friendships, romantic relationships, and decision making separate from the parents. Differentiation of self is signaled as threatened when the family system resists outside influences or treats the adult child's life choices as family decisions.
Parental identity shift: Adaptive parents reinvest in their own partnership, careers, or leisure. Enabling parents remain fused with the adult child's daily struggles, experiencing anxiety when the child is not home.
Sibling subsystem impact
Modeling effect: When younger siblings observe an adult sibling's return as a launchpad, the family narrative emphasizes temporary support. If the return becomes a cautionary tale of failure to launch, the sibling subsystem absorbs anxiety.
Resource distribution: Adaptive families equitably adjust attention and finances across all children; enabling dynamics funnel disproportionate resources to the returning adult child, breeding resentment.
Clinically, no single indicator is diagnostic. The pattern across domains and over time reveals whether the boomerang arrangement serves autonomy or reinforces enmeshment. MFTs use these indicators to guide structural interventions, reframe narratives, and contract around measurable behavior change.
Family Therapy Models for Boomerang Situations: Structural, Bowenian, and CBT Approaches
No single treatment model owns the boomerang family, but three frameworks continue to dominate clinical practice: structural family therapy, Bowenian (intergenerational) therapy, and cognitive behavioral family therapy. Each offers a distinct lens on the same core problem, an adult child re-entering a household that has already reorganized without them, and MFTs typically integrate elements from all three rather than treating them as competing schools.
Structural Family Therapy: Reorganizing Subsystems and Boundaries
Structural family therapy techniques, rooted in Minuchin's work, remain the most intuitive fit for boomerang cases because the presenting problem is almost always structural: parents and adult child are operating from an outdated map of the family. Clinical priorities include mapping the current hierarchy, identifying where subsystem boundaries have collapsed (parent-child versus spousal, adult versus minor sibling), and helping the family enact new patterns in session rather than merely discuss them. Enactments are especially useful: asking a parent and returning adult child to negotiate a household rule live in the room often reveals cross-generational coalitions or diffuse boundaries that verbal report misses.
Bowenian Therapy: Differentiation and Multigenerational Patterns
Bowen's framework shifts the focus from household logistics to the emotional process underneath them. Key concepts, differentiation of self, emotional cutoff, triangulation, and multigenerational transmission, help explain why a competent 27-year-old regresses within days of moving home, or why parents oscillate between rescuing and resenting. Genogram work is central here. Constructing a three-generation genogram often surfaces patterns the family has not connected to the current tension: parents who themselves left home late, unresolved sibling rivalries reactivated by the return, or cultural scripts about caregiving in multigenerational households. The clinical goal is not to force the adult child out, but to raise each member's capacity to stay connected without fusing.
CBT-Based Family Interventions: Reframing and Behavioral Contracts
Cognitive behavioral family approaches contribute practical tools that pair well with the more systemic models. Common targets include catastrophic thinking ("if I ask him to pay rent, he'll leave and we'll lose the relationship"), all-or-nothing framing around independence, and behavioral avoidance of difficult conversations. Structured interventions, thought records, communication skills training, and written behavioral contracts covering finances, chores, and privacy, give families concrete between-session work.
Integrating the Models in Practice
Most experienced MFTs blend approaches: structural techniques to reset the household map, Bowenian work to address differentiation and legacy patterns, and CBT tools to operationalize new agreements. For clinicians building competence in this area, AAMFT resources, peer-reviewed databases like PsycINFO and PubMed, and university-based family therapy clinics offer training materials and case literature worth reviewing before taking on complex multigenerational cases.
Session Strategies and Treatment Planning for MFTs
Structured treatment planning for boomerang family cases remains an evolving area of clinical practice, with many MFTs adapting frameworks from established family therapy models rather than following a single standardized protocol. The lack of a universally accepted manual for these cases means therapists must draw from multiple resources and tailor their approach to each family's unique configuration.
Building a Treatment Plan Framework
Effective treatment planning for boomerang families typically begins with a thorough assessment phase spanning one to three sessions. During this period, clinicians gather information about the family's history, the circumstances prompting the adult child's return, and the current relational dynamics among all household members. A genogram, the multigenerational family diagram that maps relationships, patterns, and significant events, serves as an essential tool during this phase. Constructing a genogram with the family in session often reveals recurring themes around dependency, financial support, or boundary difficulties that may span multiple generations.
Once assessment is complete, treatment goals should be collaboratively established with all participating family members. Goals frequently address boundary clarification, communication improvement, and the development of a realistic timeline for the adult child's transition toward greater independence. Session sequencing matters: many clinicians find it useful to alternate between whole-family sessions and dyadic or individual meetings, particularly when parents need space to align their expectations or when the adult child requires support in articulating their perspective without immediate parental reaction. Structural family therapy offers a particularly useful lens here, providing concrete techniques for reorganizing subsystem boundaries and restoring generational hierarchies when they have become blurred by the adult child's return.
Clinical Resources for Structured Approaches
The American Association for Marriage and Family Therapy offers a library of clinical resources and publications that can inform treatment planning. Searching their materials for terms like "boomerang families" or "multigenerational households" may yield relevant practice briefs or case discussions. Peer-reviewed databases such as PubMed and PsycINFO provide access to research on family therapy treatment plans, session sequencing, and genogram applications. Filtering searches for MFT-specific journals increases the likelihood of finding clinically applicable findings rather than purely theoretical discussions.
Several university-based MFT training programs have developed session-by-session protocols for common presenting problems. While not all of these materials are publicly available, contacting program faculty or reviewing program websites may uncover unpublished treatment guides that address multigenerational living arrangements. These academic resources often include detailed session outlines, suggested interventions for each phase of treatment, and criteria for evaluating progress. Modern family structures present a range of configurations that MFTs may encounter, and understanding how boomerang arrangements fit within that broader landscape can sharpen both assessment and goal-setting.
Integrating Demographic Context
Understanding the broader demographic trends affecting boomerang families can strengthen treatment planning. The Bureau of Labor Statistics and similar agencies publish data on young adult employment, housing costs, and household composition. While these sources do not provide clinical protocols, they help MFTs contextualize their clients' experiences within larger economic and social patterns. This awareness can inform psychoeducational components of treatment, helping families recognize that their situation reflects widespread structural factors rather than individual failure.
Adapting evidence-based practice guidelines to fit demographic realities requires clinical judgment. When economic conditions make independent living genuinely difficult, treatment plans may need to emphasize adaptive coping and household harmony rather than rapid departure from the family home.
The most productive session for many boomerang families is often the most uncomfortable one: the meeting where parents and their adult child sit together and negotiate a concrete, agreed-upon move-out timeline. When a return home has drifted from temporary to indefinite, that honest conversation becomes clinically essential, not optional.
Three-Generation Households: Interventions When Grandchildren Are Involved
When an adult child returns home with children of their own, every clinical consideration outlined for boomerang families intensifies. The grandparent subsystem, the parental subsystem, and the grandchild all occupy the same living space, and the question of who is in charge of what becomes urgent rather than theoretical. MFTs working with these families need targeted interventions that go beyond general boundary work.
Hierarchy Inversion and Its Clinical Consequences
The most common structural problem in three-generation households is hierarchy inversion: grandparents step into day-to-day parenting functions (setting bedtimes, making discipline calls, deciding what the grandchild eats) and the returning adult child quietly or resentfully cedes authority. This can happen out of genuine helpfulness, financial leverage ("I pay for groceries, so I decide what she eats"), or unresolved patterns from the adult child's own upbringing. The result is a household where the grandchild receives mixed signals about who holds executive authority, and the adult child's confidence as a parent erodes.
In session, MFTs should name this dynamic directly. Framing it as a structural issue rather than a character flaw helps all parties engage without defensiveness. The goal is not to push grandparents out of the picture but to realign the hierarchy so the adult child functions as the primary parent even while living under someone else's roof.
Defining the Grandparent Role
One of the most productive early-session exercises is asking each family member to describe the grandparent's role in concrete terms. Is the grandparent a babysitter who follows the parent's instructions? A co-parent who shares decision-making equally? A supportive bystander who offers help only when asked? Most families have never articulated this, and conflicting assumptions fuel daily friction.
Help the family negotiate explicit agreements in domains that generate the most conflict:
Discipline: Who sets consequences, and under what circumstances can a grandparent intervene?
Bedtime and routines: Whose schedule does the child follow?
Screen time: Who monitors and enforces limits?
Dietary choices: Who decides what the child eats at meals and snacks?
These may seem granular, but specificity prevents the vague goodwill of "we'll figure it out" from collapsing into resentment.
Impact on the Grandchild
Children in these households can experience confusion about authority figures and, in more conflicted families, loyalty binds where pleasing one caregiver means disappointing another. At the same time, research on attachment suggests that secure relationships with multiple caregivers can be genuinely beneficial. The clinical task is not to eliminate grandparent involvement but to ensure that involvement is coordinated rather than competitive.
MFTs should assess for signs that the child is triangulated, such as playing caregivers against each other, showing markedly different behavior with each adult, or expressing anxiety about whose rules to follow. Multicultural counseling competencies are especially relevant here, since cultural expectations around grandparent authority vary widely and can make hierarchy inversion feel appropriate to one generation while feeling intrusive to another.
Structural Mapping in Session
A whiteboard, flip chart, or digital genogram can transform an abstract conversation into a visual one the whole family can engage with. Map out the household and draw lines that represent who holds executive authority over the grandchild in each domain (meals, homework, bedtime, medical decisions). This exercise often reveals overlaps and gaps that the family has felt but never articulated.
Once the map is visible, the therapist can guide negotiation domain by domain, shifting lines of authority where needed and making agreements concrete. Families can photograph the completed map and post it at home as a reference point, reducing the odds that old patterns resurface unnoticed between sessions.
Cultural and Generational Considerations in Multigenerational Living
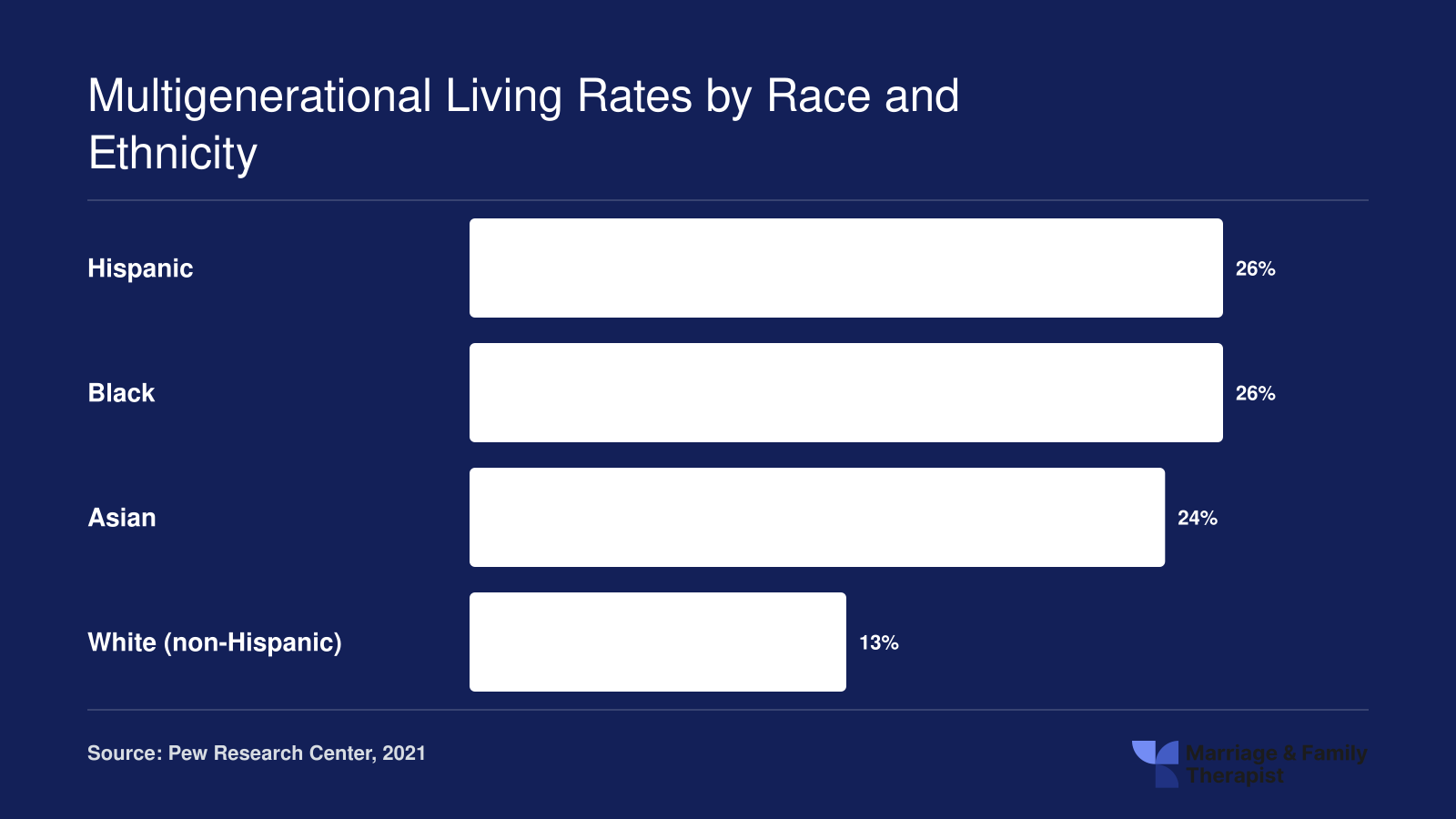
In 2021, nearly 60 million people in the United States lived in multigenerational households, representing 18 percent of the total population.1 That national average, however, conceals dramatic variation across racial, ethnic, and nativity lines. Black and Hispanic Americans each reported multigenerational household rates of 26 percent, and Asian Americans reported 24 percent, compared to just 13 percent among white Americans.1 Foreign-born adults were also significantly more likely to live in such arrangements (26 percent) compared to their U.S.-born counterparts (17 percent).1 For marriage and family therapists, these disparities underscore a critical clinical reality: the "boomerang" narrative, which frames an adult child's return home as a developmental detour or family system dysfunction, can be pathologizing when applied to communities where multigenerational coresidence is normative, expected, and often economically adaptive.
Collectivist Versus Individualist Family Norms
Many cultural traditions view multigenerational living not as a failure to launch but as a fulfillment of filial obligation, mutual caregiving, and intergenerational solidarity. In collectivist frameworks common among Asian, Latino, and many immigrant families, adult children living with parents may be seen as appropriate stewardship of family resources, a way to pool income and share caregiving duties. Roughly one-third of adults in multigenerational households in 2021 cited caregiving as a primary reason for the arrangement, reflecting roles such as caring for aging parents or supporting grandchildren.2 MFTs trained in Western developmental milestone models, which emphasize autonomy and separation in young adulthood, must consciously suspend those assumptions during assessment. Family therapy for diverse family structures offers a useful clinical lens here: the question is not whether an adult child "should" have moved out by age 25, but how the family and its members understand the current living arrangement, what functions it serves, and where tensions arise.
Cultural Humility in Practice
Cultural humility begins with curiosity rather than diagnosis. Ask families directly what multigenerational living means to them, who initiated the arrangement, and whether it aligns with their values or feels imposed by circumstance. Explore how acculturation stress may create friction: immigrant parents may expect and prefer coresidence, viewing it as natural and honorable, while U.S.-raised adult children may internalize mainstream narratives of independence and feel stigmatized by living at home. This intergenerational cultural tension, where parents and children occupy different points on the acculturation spectrum, is itself a therapeutic target. The MFT's role is to help family members articulate competing expectations, validate each perspective, and negotiate shared norms rather than enforcing a singular developmental script.
Within-Group Generational Differences
Even within the same ethnic or cultural group, generational cohort shapes expectations. First-generation immigrants may see a 30-year-old son living at home as fulfilling duty; his U.S.-born peers may see it as failure. The adult child may oscillate between pride in supporting aging parents and shame when comparing himself to friends who rent their own apartments. MFTs should normalize this ambivalence, framing it as a predictable outcome of biculturalism rather than individual pathology. Treatment planning in these cases often involves helping families co-create a narrative that honors both cultural heritage and the adult child's evolving identity, distinguishing between what the family wants from what external voices say they should want.
Multigenerational Living Rates by Race and Ethnicity
Multigenerational living is far more common in some communities than others, and these differences directly shape the clinical picture MFTs encounter during intake. Understanding baseline rates helps therapists distinguish culturally normative household structures from arrangements driven by crisis, and it prevents misapplying individualist assumptions about autonomy to families where shared living is an expected, valued practice.
Tools for Families: Contracts, Worksheets, and Conversation Guides
What specific tools can an MFT put in a family's hands between sessions to keep a boomerang situation from sliding back into old patterns? The clinical work in-session sets the frame, but structured take-home tools are what turn insight into daily behavior change. Here are four categories worth building into your treatment plan.
The Family Living Agreement
A living agreement is a written document, drafted collaboratively in session, that operationalizes the household arrangement. At minimum it should address:
Financial contribution: rent amount or equivalent (utilities, groceries, a savings match), payment schedule, and what happens if income changes
Household responsibilities: specific chores, whose car, whose groceries, pet care
Guest and overnight policies: advance notice expectations, shared spaces, romantic partners staying over
Privacy expectations: knocking, closed doors, access to bedrooms, digital privacy
Timeline for reassessment: a firm date (usually 90 days out) to review the agreement and a target move-out window if applicable
Draft it together at the whiteboard or on a shared document. When parents dictate terms, adult children comply resentfully or sabotage quietly. When the adult child co-authors the terms, ownership shifts.
Boundary-Setting Worksheet
Give each family member the same worksheet before a session. Ask them to independently list their top three non-negotiable boundaries and their top three flexible preferences. In session, map the overlaps and conflicts on a whiteboard. Teach the standard communication template: "When ____ happens, I feel ____, and I would prefer instead if ____."1 Walk through the stepwise process of identifying the limit, communicating it with I-statements, tolerating the discomfort of the other person's reaction, and defining a consequence if the boundary is ignored.2 This worksheet often becomes the raw material for the living agreement.2
The Weekly 20-Minute Check-In
Assign a standing 20-minute family meeting, same time each week. Three prompts, in order:
What's working well this week?
What needs to change or be renegotiated?
What progress did you make toward your personal goals (job search, savings, schooling, launch plan)?
This protocol prevents the slow accumulation of resentment that fuels most boomerang blowups. When violations do occur, clinicians can draw on how to set boundaries with family in therapy to help families calibrate their responses, including strategies like shortening conversations or adjusting access to shared resources.3
Published Clinical Instruments Worth Adapting
Several established tools translate well to this population: genogram software (GenoPro, Genogram Analytics) for visualizing three-generation patterns, the FACES-IV (Family Adaptability and Cohesion Evaluation Scale)2 to measure cohesion and flexibility before and after intervention, and role-mapping exercises from structural family therapy literature to make invisible subsystem dynamics concrete on paper. Ready-made boundary worksheets are also available through clinical therapy marketplaces for practitioners who want a quick starting point.4
Common Questions About Family Therapy for Boomerang Families
Families navigating a boomerang transition often have pressing questions about when to seek help, what to expect in therapy, and how to maintain healthy relationships under one roof. Below are answers grounded in the structural, Bowenian, and cognitive behavioral frameworks discussed throughout this guide.
When your adult daughter moves back home, when should the family seek therapy?
Consider therapy when recurring arguments, resentment, or emotional withdrawal begin to disrupt the household. If attempts at setting ground rules repeatedly break down, or if the returning adult child or parents show signs of anxiety, depression, or chronic conflict, a licensed marriage and family therapist can facilitate productive conversations before patterns become entrenched. Early intervention is typically more effective than waiting for a crisis.
What family therapy models work best for adult children moving back home?
Structural family therapy is especially effective because it directly addresses hierarchy and subsystem boundaries, helping families clarify roles when an adult child reenters the home. Bowenian therapy supports differentiation of self, so the returning adult can maintain autonomy while staying emotionally connected. Cognitive behavioral approaches are useful for identifying and restructuring unhelpful thought patterns, such as a parent's belief that any boundary setting equals rejection.
How do therapists help families set boundaries when an adult child returns?
Therapists guide families through explicit boundary negotiations covering finances, household responsibilities, privacy, and social expectations. As Jim Daly advised in a July 2026 column for Focus on the Family, treating the returning adult as a boarder with clear rules for order, privacy, and respect helps distinguish them from minor children in the home. An MFT facilitates this process with structured conversations and, often, a written household agreement.
How do you differentiate healthy interdependence from enabling dependence in multigenerational households?
Healthy interdependence features mutual contribution, clear timelines, and progress toward the adult child's personal goals, whether financial stability, education, or career development. Enabling dependence, by contrast, involves the family absorbing responsibilities the adult child could manage, reducing their motivation to become self sufficient. Therapists assess factors like financial contribution, emotional functioning, and whether the living arrangement supports or stalls the adult child's developmental trajectory.
What is the impact on younger siblings when an adult child moves back home?
Younger siblings, especially teenagers, may experience confusion about household rules if the returning adult operates under a different set of expectations. They can also feel displaced or resentful if parental attention shifts. Structural family therapy emphasizes maintaining clear distinctions between the parental, adult child, and minor child subsystems. Therapists help parents communicate age appropriate expectations so younger children understand that different rules reflect different developmental stages, not favoritism.
When should a family seek professional help for boomerang living situations?
Professional help is warranted when the family cannot resolve disagreements about finances, chores, or privacy on their own, or when the arrangement triggers regression in the adult child's independence. Other indicators include escalating tension between the parents themselves, signs of mental health distress in any family member, or a pattern in which the adult child's return becomes indefinite without a transition plan. An LMFT can assess whether the situation is adaptive or enabling and design interventions accordingly.