What you’ll learn in this article…
- Perimenopause can start in the early-to-mid 40s, lasting years.
- CBT shows a pooled effect size of 0.60 for menopausal quality of life.
- Vermont providers show training gaps in updated menopause treatment guidelines.
Evidence-based frameworks, assessment tools, and session strategies for MFTs working with couples and families navigating perimenopause and menopause.

A July 2026 investigation by Seven Days found that women in Vermont are waiting weeks or months for appointments to discuss estrogen therapy, with providers showing gaps in training and uneven adoption of updated menopause treatment guidelines.1 For marriage and family therapists, this access problem does not stay inside a medical office. It shows up in your session room as escalating couples conflict, unexplained mood shifts, sleep-deprived parenting, and sexual health complaints that neither partner fully understands.
Menopause reshapes the entire relational system. Partners misread irritability as rejection, adolescents lose a predictable caregiver, and extended family members default to dismissal. When the medical system is slow to respond, the therapeutic relationship often becomes the first place a client can make sense of what is happening. This dynamic closely parallels what MFTs encounter in postpartum depression couples therapy, where hormonal and relational factors are similarly entangled and the presenting distress is easily misread as purely psychological.
The clinical stakes are concrete: misattributing hormonally driven distress to purely psychological causes can stall treatment for months and erode the therapeutic alliance in the process.
Perimenopause is the transitional phase when the ovaries begin producing less estrogen and progesterone, typically starting in the early-to-mid 40s, though it can begin earlier. It is not a single event but a stretch of hormonal fluctuation that may last anywhere from four to ten years. Menopause itself is defined retrospectively: 12 consecutive months without a menstrual period. Postmenopause refers to every year after that milestone. Marriage and family therapists need this vocabulary not because they diagnose or treat the physiology, but because speaking the same language as a client's physician, OB-GYN, or nurse practitioner makes interdisciplinary collaboration far more effective.
Clients in perimenopause or menopause rarely walk in and say, "I think my hormones are affecting my marriage." Instead, MFTs encounter a constellation of symptoms that can mimic or overlap with anxiety, depression, ADHD, and relational distress. The most clinically relevant clusters include:
Because these symptoms overlap with diagnosable mental health conditions, it is easy to misattribute them entirely to psychological causes. This dynamic closely resembles the challenge MFTs face when postpartum depression enters couples therapy, where hormonal and relational factors are similarly entangled.
Not every mood shift during perimenopause warrants a psychiatric diagnosis, and not every presentation is "just hormones." MFTs should watch for referral red flags that suggest a client's distress exceeds what a normal hormonal transition would explain. Suicidal ideation, severe functional impairment at work or home, psychotic features, or a rapid decline that does not track with the gradual nature of hormonal shifts all call for prompt collaboration with a prescriber or mental health specialist. At the same time, clinicians should avoid dismissing significant distress as an inevitable part of aging.
A July 2026 report in Seven Days illustrated this point vividly.1 Kirsten Berggren, a family medicine nurse practitioner in Vermont who began experiencing perimenopause symptoms at age 49, started using an estrogen patch on a colleague's recommendation and felt noticeable relief within three days. Her case is a reminder that hormonal treatment can shift a client's presentation with striking speed. An MFT who spends months working on what appears to be treatment-resistant anxiety or relational irritability may be addressing a symptom whose root cause responds rapidly to medical intervention.
This does not diminish the value of therapy. Relationship patterns that formed during years of untreated symptoms do not vanish when a patch is applied. But it does mean that MFTs who stay curious about the biological dimension, and who ask direct questions about menstrual changes, hot flashes, and sleep quality, will arrive at a more accurate clinical picture and help clients access the right combination of care.
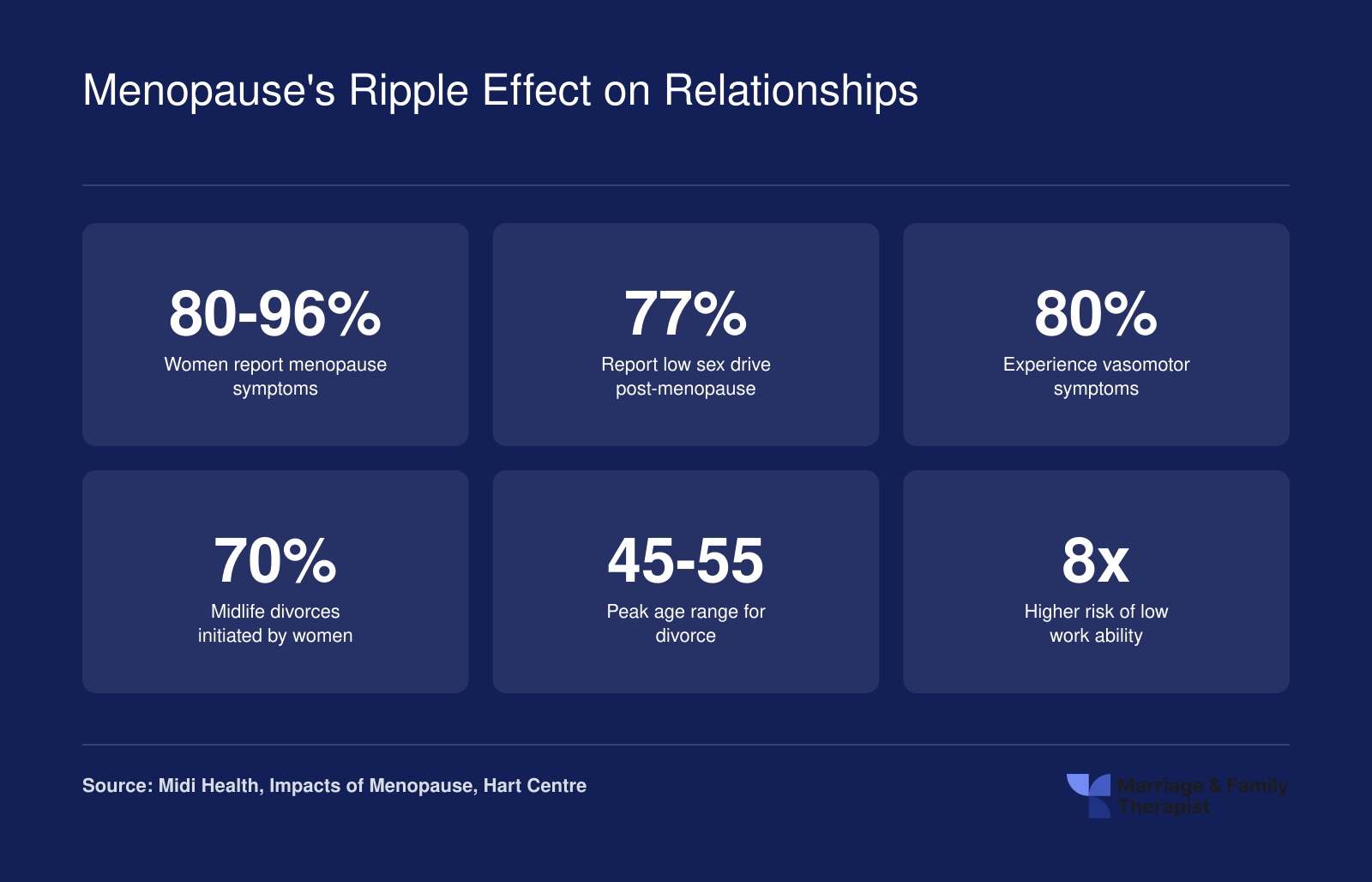
Menopause is far more than a medical event. The numbers below reveal how hormonal transitions reshape intimate partnerships, family dynamics, and daily functioning, making a compelling case for why every MFT should treat menopause as a relational issue that belongs squarely in clinical practice.
A thorough assessment is the foundation of effective menopause-informed therapy, and most standard intake protocols miss the hormonal dimension entirely.
Adding a short cluster of menopause-aware questions to your existing intake process costs little time and yields significant clinical insight. Consider asking:
For the partner or co-parent, direct questions matter equally:
These questions normalize the topic, signal that the therapist views physical health as part of relational health, and open a channel for conversations the couple may have been avoiding.
The genogram is an underused tool for menopause work. When you map menopausal transitions across generations, patterns emerge: families often carry unspoken scripts about aging, sexuality, and gender roles that shape how a client interprets her own experience. Note ages at menopause onset, documented symptoms, and any history of hormone therapy use or refusal. These markers help both therapist and client see a perimenopausal transition as a life-cycle event with family context, not an isolated personal failure.
Organizing your evaluation around four domains keeps the assessment comprehensive without becoming unwieldy:
Three instruments are particularly well suited to MFT assessment contexts.
The Menopause Rating Scale (MRS) is an 11-item, validated self-report tool covering somatic, psychological, and urogenital or sexual symptom domains.1 It carries a Cronbach's alpha of 0.87, indicating strong internal consistency, and has been used in couples and relational research settings.2 The MRS is available in multiple languages, including Chinese, Portuguese, Czech, and Indonesian, which broadens its utility with multicultural therapy competencies for marriage and family therapists working across diverse client populations.3 Non-commercial clinical use is possible through a request process managed by the copyright holder and Mapi Research Trust; it is not freely downloadable without that step.4
The Female Sexual Function Index (FSFI) is a 19-item tool assessing desire, arousal, lubrication, orgasm, satisfaction, and pain. It is widely used in sexual health research and gives MFTs a structured way to open conversations about specific dimensions of sexual functioning rather than relying on broad self-report. Licensing arrangements vary, so therapists should verify current access terms before use.
The Dyadic Adjustment Scale (DAS) assesses relationship satisfaction across consensus, cohesion, affection, and satisfaction subscales. It is a purchase-required instrument but remains one of the most widely validated measures of couple functioning available, making it a useful pre- and post-treatment benchmark when menopause-related relational distress is the presenting concern.
Using even one of these instruments alongside your clinical interview gives you a structured baseline, supports outcome tracking, and communicates to clients that their experience is taken seriously as a clinical matter.
A 2024 systematic review of 30 studies found that cognitive behavioral therapy produced meaningful improvements in quality of life for menopausal women, with a pooled effect size of 0.60 and a confidence interval ranging from 0.40 to 0.85.1 That is a clinically significant finding, and it gives MFTs a strong empirical foundation for the work they are already positioned to do.
CBT has the deepest evidence base for menopause-related distress. The MENOS protocol, developed specifically for menopausal symptoms, delivers measurable results in just four to six sessions, making it practical for outpatient MFT settings.3 Across 16 studies involving roughly 910 participants, CBT showed reductions in anxiety and depression as well as improved memory complaints.1 Both the National Institute for Health and Care Excellence and the North American Menopause Society have formally recommended CBT for menopause-related symptoms, including vasomotor complaints like hot flashes.2
For couples work, CBT adapts naturally. Catastrophic thinking about aging, fear of becoming unattractive, or automatic assumptions that a partner's withdrawal signals the end of desire are all cognitive distortions that respond to standard CBT restructuring techniques. The therapist can run individual CBT components while simultaneously addressing the relational patterns those distortions produce. MFTs looking for a broader orientation to evidence-based family therapy modalities will find that CBT sits comfortably alongside systemic and attachment-focused approaches.
Menopause often triggers precisely the attachment threats EFT was designed to address. A partner who pulls away during a woman's mood fluctuations or sleep disruption may be responding out of confusion rather than rejection, but the impact on attachment security can be significant. EFT's cycle-interruption work helps both partners name the fear underneath the behavior: one person pursuing reassurance, the other withdrawing to avoid conflict.
While large-scale EFT trials focused specifically on menopausal couples are limited, EFT's efficacy with distressed midlife couples is well established. The menopause transition maps cleanly onto EFT's core framework of vulnerability, protest, and disconnection, and many clinicians report that naming the hormonal transition as a shared stressor, rather than a character flaw, accelerates the softening process.
Acceptance and Commitment Therapy is particularly well suited to the identity dimension of menopause. Many clients arrive struggling not just with symptoms but with grief: grief over fertility, over a body that felt predictable, over a version of themselves they associated with vitality or sexual confidence. ACT does not ask clients to feel better about those losses. It asks them to hold the discomfort without letting it dictate behavior.
In couples contexts, ACT can shift the conversation from performance-based intimacy, where sex must look a certain way to count, toward values-based intimacy, where connection, curiosity, and presence become the organizing principles. That reframe often reduces the pressure that makes sexual avoidance more likely.
Systemic family therapy models and sex therapy integration deserve a place alongside these individual-focused approaches. A systemic lens keeps the therapist from over-locating the problem in the menopausal woman while ignoring family patterns that predate the transition. Sex therapy frameworks provide specific tools for addressing genitourinary symptoms, desire discrepancy, and communication about changing sexual needs.
The practical reality is that few presentations call for a single modality. A skilled MFT might use CBT to address hot-flash-related anxiety, EFT to repair attachment ruptures, ACT to support identity adjustment, and systemic thinking to assess whether family roles are constraining everyone's ability to adapt. These approaches are not competing frameworks. They are complementary lenses, and menopause is a transition complex enough to benefit from all of them.
Effectively supporting clients through menopause means matching the therapeutic approach to the core relational and psychological disruption. This quick-reference guide distills four evidence-supported modalities across key dimensions to help MFTs make deliberate, client-centered choices.
MFTs who want a broader comparison of marriage and family therapy modalities can use that resource alongside this section to triangulate the best fit for each presenting concern.
Sexual health concerns often surface mid-treatment or remain unspoken entirely. Menopause brings physiological changes (vaginal dryness, tissue thinning, shifts in libido) that affect intimacy, yet many couples hesitate to raise the topic, and therapists sometimes mirror that avoidance. The uneven access to hormone therapy documented in Vermont underscores a national pattern: clients may arrive without a provider who has named what is happening or discussed options. The MFT may be the first professional to validate that physical changes are real, treatable, and worthy of attention.
Normalizing the conversation begins with a clear, inviting opener. Try phrasing such as, "I want to check in about how physical changes have affected your intimate life. Is that something you would be willing to explore together?" This signals permission, frames intimacy as part of relational health, and invites both partners into the dialogue. Many clients report relief when a therapist initiates the topic, removing the burden of disclosure.
Concrete interventions help partners communicate about what has changed and how to adapt. Couples therapy communication patterns matter here: the way a therapist frames an opening question can determine whether partners engage or withdraw.
MFTs operate within a clear scope-of-practice boundary. You can educate clients about options such as over-the-counter vaginal lubricants, vaginal estrogen (a prescription treatment), and pelvic floor physical therapy as resources to explore with a physician. You should not prescribe, recommend specific brands or dosages, or suggest that a particular medical treatment is necessary. Frame your role as informed advocacy: "Some women find relief through lubricants or vaginal estrogen. I encourage you to discuss these options with your primary care provider or gynecologist." This respects the MFT's expertise in relational dynamics while honoring the physician's role in medical decision-making. Reviewing your LMFT continuing education requirements by state can help you identify training opportunities that sharpen clinical competency in areas like sexual health and integrated care.
Given the care gaps described in the Vermont reporting, assume that some clients have not received menopause-specific counseling from their medical team. Normalizing language matters: "What you are describing, hot flashes, sleep disruption, changes in arousal, are common during perimenopause. There are treatments that can help. Have you had a chance to talk with your doctor about menopause?" This opens a referral pathway and validates the client's experience without overstepping clinical boundaries.
The family systems literature has largely overlooked menopause as a clinical variable, leaving MFTs without a clear framework for the household dynamics it generates.
One of the most underexamined intersections in family therapy is the simultaneous onset of adolescent puberty and parental perimenopause. A teenager navigating mood swings, identity formation, and emotional intensity is sharing a household with a parent experiencing their own hormonal volatility, disrupted sleep, and shifting sense of self. Each party can misread the other's distress as hostility or rejection, and conflict that looks purely interpersonal often has a biological dimension that no one has named.
Families in this situation benefit when the therapist introduces a normalizing frame early. Explaining that two genuine neurobiological transitions are occurring at once does not excuse behavior from either party, but it does reduce the personalization that fuels the sharpest arguments. Teens frequently assume a parent's irritability is directed at them. Naming menopause in a family session, plainly and without clinical jargon, gives adolescents a more accurate explanation and tends to lower their defensive posturing. MFTs who work regularly with younger clients can draw on child and adolescent counselor career path resources to deepen their developmental framing here.
Menopause rarely arrives in isolation. Many women in perimenopause are simultaneously providing care for aging parents while raising children still at home. This sandwich generation pressure compounds hormonal symptoms in ways that are easy for a therapist to misread as clinical depression or relationship dissatisfaction alone. Caregiver burnout, grief over a parent's decline, and the physical demands of midlife can all amplify what estrogen depletion is already doing to sleep, concentration, and emotional regulation.
When a client presents with exhaustion and relational withdrawal, a thorough assessment includes questions about caregiving load and extended family obligations, not just couple-level dynamics.
Several approaches translate well into this context:
Positioning menopause as a family-level event rather than an individual pathology is one of the more meaningful reframes an MFT can offer, and the field is only beginning to build the tools to do it well.
Menopause is not a universal experience, and the clinician who treats it as a single script does a disservice to clients whose race, ethnicity, sexual orientation, gender identity, and socioeconomic context fundamentally shape both symptom burden and access to care. Data from the United Kingdom show that Black and minoritized women face delayed diagnosis at a rate of 45 percent, compared to 31 percent for white women, and use hormone therapy at half the rate (8 percent versus 15 percent), a disparity that reflects both structural barriers and the compounding effects of cultural invisibility.1 Marriage and family therapists working in the United States encounter analogous gaps: Black and Latina women report more severe and earlier-onset vasomotor symptoms, yet their concerns are often dismissed or misattributed to stress or mental illness, delaying medical referral and magnifying relational strain.
Cultural attitudes toward menopause vary widely, and these narratives shape how clients present in therapy. Some traditions frame menopause as liberation, a relief from fertility and contraception, while others cast it as loss, decline, or invisibility. In many Asian cultures, menopause is rarely discussed aloud, leaving women to interpret symptoms in isolation. Among some African American communities, menopause is acknowledged but may be under-medicalized due to historical mistrust of the healthcare system. MFTs must recognize that a client's emotional response to perimenopause is inseparable from the cultural stories she has internalized, and that her willingness to pursue hormone therapy, lifestyle changes, or even couples work around intimacy may be influenced by messages about aging, femininity, and worthiness. Multicultural therapy competencies for marriage and family therapists offer a useful framework for approaching these conversations with appropriate humility and skill.
LGBTQ+ menopause experiences remain markedly under-represented in research, and what little data exist confirm distinct clinical considerations.2 Sexual minority women and non-binary people enter perimenopause at roughly the same age as heterosexual cisgender women (mean onset around 43.6 to 43.7 years, completion between 47.5 and 49.8 years), but their needs diverge sharply.2 Lesbian couples may navigate simultaneous menopause, compounding sleep disturbances and mood shifts in a system with no partner buffer. Transgender men on testosterone may still experience perimenopausal symptoms if ovaries remain; the 2022 WPATH Standards of Care note that masculinizing hormone therapy does not reliably suppress ovarian cycling until oophorectomy.3 For non-binary clients, menopausal body changes, particularly breast tenderness, weight redistribution, and changes in body hair, can trigger dysphoria that clinicians miss if they assume all menopausal clients are cisgender women. Recent clinical guidance published in 2026 emphasizes that trans and gender diverse individuals aged 40 to 70 report feeling invisible in menopause care, and that provider training lags far behind patient need.4 LGBTQ+ affirming mental health care resources can help MFTs build the competency needed to serve these clients well.
The Seven Days article on Vermont's uneven estrogen therapy access illustrates a national pattern: rural and underserved communities face provider shortages, outdated training, and insurance barriers that leave hormone therapy out of reach for many. Low-income women, disproportionately women of color, may lack paid sick leave to attend appointments, affordable childcare during clinic hours, or insurance that covers compounded bioidentical hormones. MFTs in community health centers, telehealth practices, and rural settings are often the first or only mental health provider a client sees, making early recognition and warm handoffs to primary care or gynecology essential.
Avoid assumptions about a client's relationship to menopause based on demographics. Instead, use open-ended questions: How do you understand what's happening in your body? What messages did you grow up hearing about menopause? Who in your family or community has talked about this transition? Incorporate cultural humility frameworks, acknowledging the limits of your own knowledge and inviting clients to educate you. When collaborating with medical providers, advocate explicitly for clients from marginalized groups, naming disparities and requesting second opinions when symptoms are minimized. The goal is not to become an expert in every cultural script, but to create space for each client's lived experience and to recognize when systemic inequity is shaping both symptom presentation and treatment access.
Interdisciplinary collaboration means coordinating care between you and medical professionals who address the physiological dimensions of menopause. As an MFT, your role is not to prescribe or manage hormone therapy, but to recognize when clients need that expertise and to maintain a trusted referral network.
You should compile a list of local providers who understand menopause care, including OB-GYNs, endocrinologists, and NAMS-certified practitioners (those credentialed by The Menopause Society). Refer clients when you see symptoms that may surpass typical hormonal adjustment, such as major depressive disorder that does not respond to your relational interventions. Also refer for cases of medical menopause, such as surgical removal of ovaries or chemotherapy-induced changes, and whenever a client expresses interest in hormone replacement therapy (HRT). Having these connections in place before you need them allows you to act quickly while keeping the family system at the center.
The AAMFT Code of Ethics (2015) requires that you practice within your boundaries of competence (Standards 3.10 and 3.11).1 You may discuss the existence of medical options, such as different forms of HRT, as part of normalizing the experience and encouraging informed decision-making, but you must stop short of recommending a specific treatment. Client autonomy is a core principle; your job is to help clients gather information and ask the right questions of their medical providers.1 If you are unsure whether a conversation crosses into medical advice, seek supervision immediately.2 The upcoming 2026 Code of Ethics update reinforces that interdisciplinary consultation is an ongoing requirement, not a one-time check.3
When coding diagnoses, be precise. If menopause-related stress contributes to relational conflict but does not meet the threshold for a mood disorder, consider a relational V-code (e.g., Z63.0 for problems in relationship with spouse or partner) and note menopause as a contextual factor in your clinical documentation. If a client shows depressive symptoms that are best explained by hormonal changes, an adjustment disorder code may fit; reserve major depressive disorder for cases where the severity and duration align with that diagnosis. Accurate coding protects your clients and supports ethical billing. If navigating how relational stress from a life transition like menopause intersects with couple dynamics, communication pitfalls couples therapists should address can inform how you document and prioritize presenting concerns.
Before you advertise yourself as a menopause-informed therapist, seek continuing education.2 The North American Menopause Society offers a Certified Menopause Practitioner credential for allied health professionals, which provides foundational knowledge without overstepping scope. For deeper work on sexual health, AASECT certification integrates biopsychosocial approaches. Any new area of practice requires not only coursework but also supervision and consultation until you have achieved full competence, as mandated by the profession's competence-based scope of practice.2
Marriage and family therapists are increasingly encountering menopause and perimenopause as factors in the clinical presentations they treat. Below are direct, practical answers to questions that come up frequently as clinicians build competence in this area.
How can MFTs start integrating menopause-aware care into their practice this week? Begin by auditing your intake forms and adding one straightforward question about hormonal changes, then identify a local provider to add to your referral network. This simple week-one action moves you from awareness to action.
Menopause is a systemic, relational issue, not solely a medical one, and uneven access to informed care means therapists often become the first point of meaningful guidance. When clients cannot get timely, knowledgeable medical support, MFTs can normalize the conversation, validate the impact on relationships, and advocate for integrated treatment. Building a menopause-informed practice does not require a new specialization. It starts with a deliberate shift in your clinical lens and a commitment to bridging the gaps your clients face every day. experienced MFTs who invest in continuous clinical improvement are better positioned to serve this often-overlooked population with the competence and confidence the work demands.