Evidence-Based Interventions Therapists Use to Address These Pitfalls
When couples therapists encounter destructive communication patterns, they draw on structured treatment models backed by decades of clinical research. Four major evidence-based approaches have demonstrated measurable success in helping couples replace criticism, contempt, stonewalling, and defensiveness with healthier interaction patterns. Each modality offers distinct mechanisms of change, targets specific pitfall patterns most effectively, and has produced outcome data that inform clinical decision-making.
Emotionally Focused Therapy (EFT): Attachment Restructuring for Withdrawal and Stonewalling
Emotionally Focused Therapy targets the attachment injuries and emotional disconnection that fuel patterns like stonewalling and defensive withdrawal. The core mechanism is attachment restructuring: helping partners access and express underlying vulnerable emotions (fear of abandonment, shame about inadequacy) that drive their communication defenses. EFT therapists guide couples through structured conversations that de-escalate blame cycles and create new bonding experiences.
EFT shows particularly strong outcomes for distressed couples.1 Published meta-analytic data from 1999 reported effect sizes around 1.3, indicating that the average couple treated with EFT moved from the 10th percentile of relationship satisfaction to approximately the 90th percentile. This modality excels when stonewalling or emotional withdrawal stems from attachment anxiety rather than simple skill deficits. Recovery rates in randomized trials consistently place 70 to 75 percent of couples in the recovered or significantly improved range after treatment.
Integrative Behavioral Couple Therapy (IBCT): Acceptance and Change for Communication Problems
Integrative Behavioral Couple Therapy blends traditional behavioral skills training with acceptance-based strategies. The core mechanism balances two pathways: teaching concrete communication and conflict-resolution skills while simultaneously helping partners accept differences that cannot or need not change. IBCT therapists teach couples to observe their interaction patterns without judgment and to build empathy around each partner's emotional sensitivities.
IBCT is particularly well-suited for couples with entrenched communication problems where partners have tried and failed to change each other's behavior. A 2018 meta-analysis reported effect sizes around 0.76 for IBCT interventions, with significant gains maintained at two-year follow-up.2 This modality addresses criticism and contempt by shifting focus from blame to understanding the context and function of each partner's behavior.
Behavioral Couple Therapy (BCT) and CBT-Based Approaches: Skills Training for Couples Needing Structure
Traditional Behavioral Couple Therapy and cognitive-behavioral approaches emphasize direct communication skills training: active listening, I-statements, conflict-resolution protocols, and homework assignments to practice new behaviors. The core mechanism is behavioral exchange, where couples learn to increase positive interactions and manage conflict constructively through rehearsed techniques.
BCT works best for couples who lack basic communication competencies rather than those with deep attachment wounds. A 2003 meta-analysis found effect sizes around 0.82 for behavioral interventions, with strongest outcomes when both partners actively engage in skill practice between sessions.3 This approach directly targets defensiveness by teaching partners to express needs without blame and to validate each other's perspectives before problem-solving.
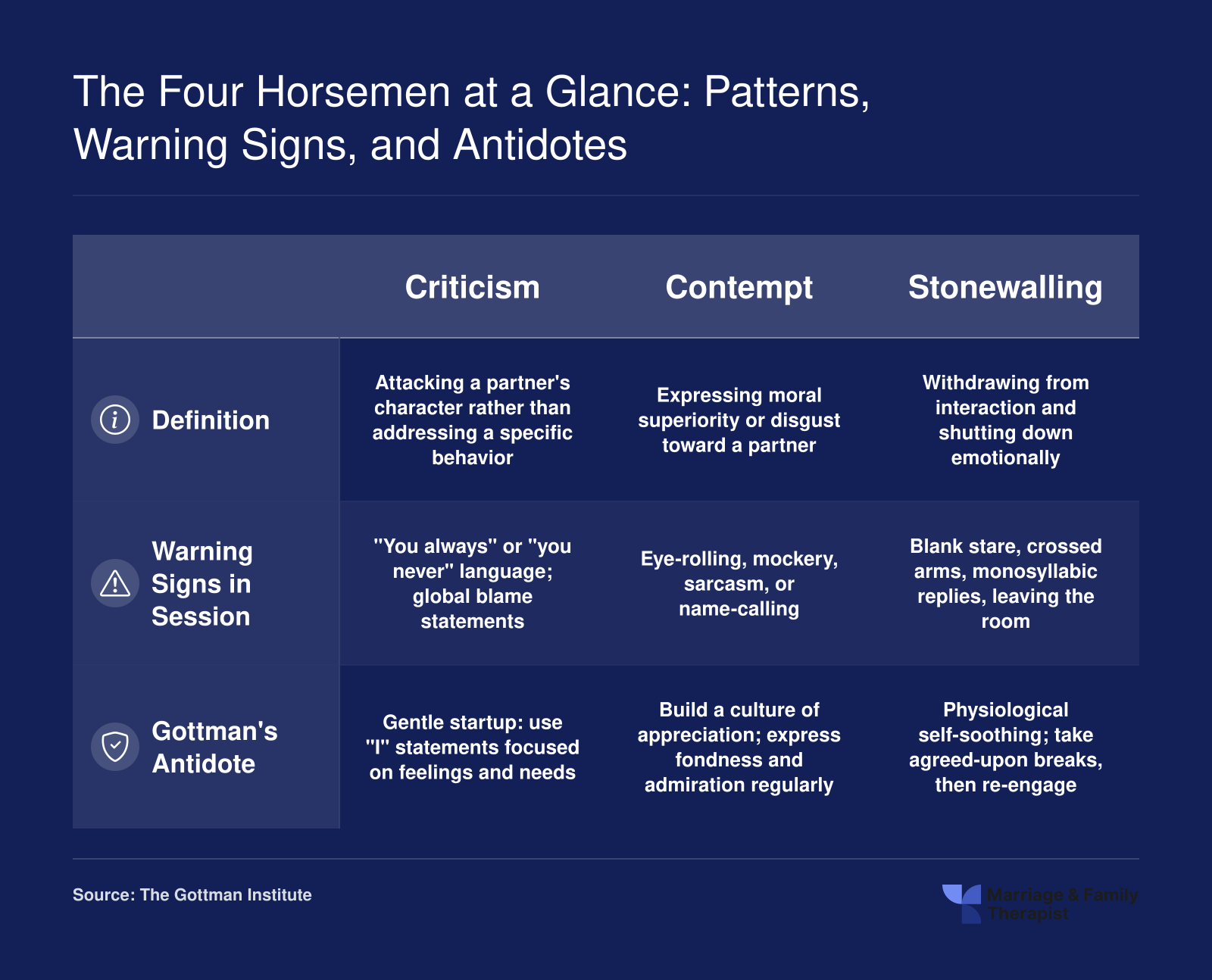
The Gottman Method: Targeting the Four Horsemen Directly
The Gottman Method integrates research on stable versus distressed couples into a structured intervention framework. Core mechanisms include teaching couples to recognize and interrupt the Four Horsemen (criticism, contempt, defensiveness, stonewalling), build a culture of appreciation and respect, and manage perpetual conflicts without damage. Gottman-trained therapists use Gottman method assessment tools like the Sound Relationship House questionnaires to identify specific areas of vulnerability, then tailor interventions to each couple's profile.
The Gottman Method is particularly effective for criticism and contempt cycles because it directly trains couples to replace harsh startup and contemptuous nonverbals with softened communication. While large-scale randomized controlled trials for the complete Gottman Method are fewer than for EFT or IBCT, published studies show satisfaction improvements and reduced negative communication in 60 to 70 percent of treated couples. The method's strength lies in its practical, psychoeducational format that gives couples concrete tools they can apply immediately.
Integration in Practice: Therapists Are Not Locked Into One Model
Most experienced couples therapists integrate techniques across modalities rather than adhering rigidly to a single approach. An MFT might use Gottman-based psychoeducation to help a couple recognize their Four Horsemen patterns, then apply EFT techniques to access the attachment fears beneath a partner's stonewalling, and finally assign IBCT-style acceptance exercises when partners disagree on parenting philosophies. Research on treatment integration suggests that flexibility improves outcomes, particularly when couples present with multiple pitfall patterns or when one modality alone does not produce sufficient progress. Aspiring therapists benefit from training in multiple marriage and family therapy modalities, allowing them to match interventions to each couple's unique communication challenges and relational context.