IFS Training and Certification Pathway
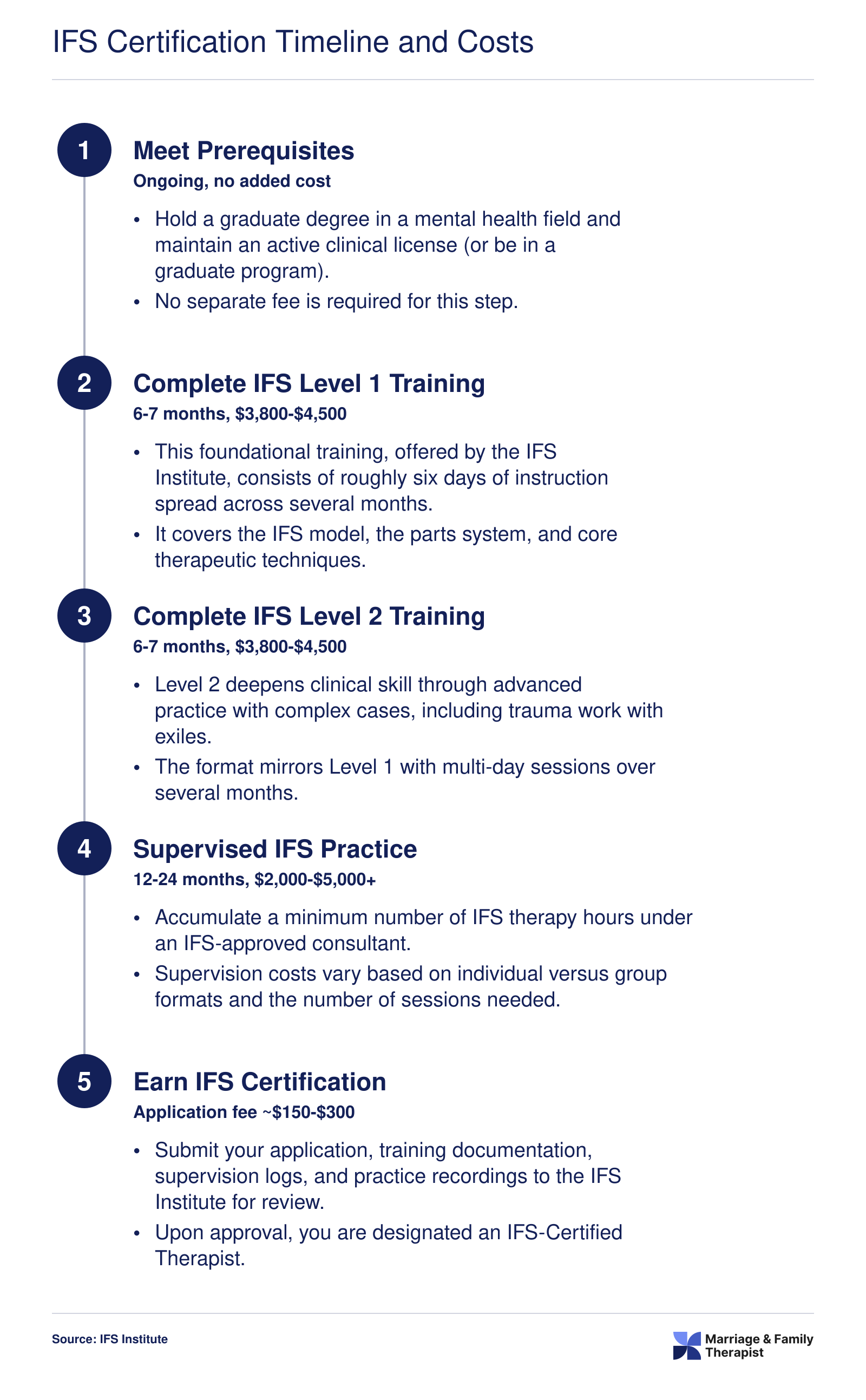
Becoming a certified IFS therapist requires a structured progression through the IFS Institute's training levels, plus supervised clinical practice. The pathway is rigorous, but it is designed so that working clinicians can complete it alongside an active caseload. Here is what each stage involves and what you should budget in time and money.
Level 1: Foundational Training
Level 1 is the gateway to every other IFS credential. It spans 91 contact hours delivered across several months and covers the core model, including the Self, the three categories of parts (managers, firefighters, and exiles), and the fundamental therapeutic steps.1 Formats include online, hybrid, and fully in-person options, giving you flexibility depending on your schedule and learning style. To receive a Certificate of Completion, you must attend at least 76 of the 91 hours.
Eligibility is limited to mental health professionals, which includes licensed therapists (LMFTs, LPCs, LCSWs, psychologists) as well as graduate-level trainees working toward licensure.3 Coaches and other non-clinical practitioners sometimes seek admission, but applicants should check the IFS Institute's current general application requirements to confirm eligibility. If you are still exploring how to become a licensed marriage and family therapist, completing Level 1 during your graduate program can give you a head start.
Cost in North America currently ranges from roughly $3,990 to $5,300, with variation based on format and location.4 Continuing education credit for the full 91 hours is available through The Institute for Continuing Education, which makes this investment count toward state CE requirements for most licensed clinicians.
Level 2: Deepening Practice
After completing Level 1, therapists can move to Level 2, which focuses on applying the model to more complex clinical scenarios such as trauma processing with exiles and working with protective parts that resist unburdening. Tuition falls between approximately $2,550 and $2,950.4 This level builds the clinical depth you will need before pursuing certification.
Level 3: Advanced Training
Level 3 requires completion of both prior levels and addresses advanced topics, including working with legacy burdens, couples, and entrenched systems. Expect to invest between roughly $2,700 and $2,900 for this stage.4
The IFS-Certified Therapist Designation
A Certificate of Completion from any training level is not the same as certification. The IFS-Certified Therapist credential is a separate designation issued by the IFS Institute. It requires, at minimum, completion of Level 1 plus documented supervised practice hours using the model under an approved IFS consultant. Many candidates also complete Level 2 or Level 3 before applying, though Level 1 is the stated minimum training prerequisite.
The total timeline from your first Level 1 session to earning the certified therapist designation typically runs two to four years. Factors that affect pace include how quickly you accumulate supervised practice hours, how soon you enroll in subsequent levels, and your consultant's availability.
Total Investment
When you add up tuition across all three levels, the training alone can range from roughly $9,240 to $11,150 before factoring in consultation fees, application costs, and any travel for in-person sessions.4 Costs may differ if you train outside North America; in Australia, for example, Level 1 fees are estimated around AUD 6,800 and remain subject to review.5 Weighing this investment against long-term earning potential is worthwhile, and reviewing current marriage and family therapist salary data can help you make an informed decision.
Continuing Education Credit
IFS training hours generally qualify for CE credit accepted by most state licensing boards for LMFTs, LPCs, and LCSWs. Verify with your specific state board, as acceptance policies can vary. For therapists who need to fulfill CE obligations anyway, stacking IFS training with renewal requirements is a practical way to maximize both your clinical skill set and your licensure compliance.