In-law dynamics, not infidelity, top Indian-American couples' intake concerns.
Asian American adults use mental health services at half the national rate.
No major EFT or Gottman trial has specifically studied Indian-American couples.
Indian-American couples enter therapy with a distinct constellation of stressors that standard evidence-based models rarely address: migration-related identity shifts, non-negotiable family obligations across generations, and deep stigma around mental health help-seeking. When a therapist trained exclusively in Western individualist frameworks encounters a couple navigating in-law involvement or arranged-to-love marriage transitions, the mismatch can derail treatment before trust is even established.
On July 16, 2026, LeapHope, a Brooklyn-based online mental health platform, announced an expansion of its specialist network to serve Indian-origin families across the United States.1 The move signals rising demand for clinicians who understand collectivist family structures, multilingual communication patterns, and the cultural weight of shame in disclosing relational conflict.
Culturally competent marriage and family therapy career paths for those serving Indian-American couples require more than cursory nods to tradition. Effective practice demands fluency in how family hierarchy shapes decision-making, how mental health stigma silences distress, and how Western therapeutic assumptions about autonomy and directness can alienate the very clients they aim to help.
Why Indian-American Couples Need Culturally Competent MFTs
Cultural competence in marriage and family therapy means more than speaking a second language or nodding at a client's traditions. It means a therapist understands how a specific community defines the self, the marriage, the family, and the very concept of asking for help. For Indian-American couples, that distinction is not cosmetic. It shapes whether therapy works at all.
A Population Too Large to Overlook
The Indian-American community has grown by roughly 174 percent since 2000, reaching approximately 5.2 million people as of 2023.1 About two-thirds are immigrants, and the remaining third were born in the United States. That split matters clinically: immigrant Indian Americans marry at a rate around 77 percent, compared to just 35 percent among U.S.-born Indian Americans,2 a gap that reflects vastly different degrees of acculturation, family expectation, and relationship pressure. Overall, married-couple households account for 73 percent of Indian-American family units, compared to 48 percent nationally.3 Roughly 80 percent of Indian Americans marry within their own ethnic community, and about 20 percent of couples are intermarried.3 These are not abstract numbers. They describe a community with high rates of formal partnership, significant intergenerational friction around how those partnerships form, and a relatively small but growing population navigating separation and divorce.
The Utilization Gap
Despite this population size and these relationship pressures, Indian-American and broader Asian-American communities consistently underutilize mental health services. Research accessible through the U.S. National Library of Medicine points to structural barriers including stigma, limited availability of culturally matched providers, and a fundamental mismatch between Western therapeutic models built around individual autonomy and the collectivist value systems that govern many South Asian families. When a therapeutic framework assumes that personal fulfillment is the primary goal of a healthy marriage, it can feel alienating, or even offensive, to a couple whose family and community loyalty are central to their identity. Cultural humility in marriage and family therapy is not optional for MFTs serving this population; it is the foundation on which every intervention rests.
The Market Is Responding
Services built specifically for this population are emerging to fill the void. In July 2026, LeapHope, an online mental health platform founded by Shwati Singh and based in Brooklyn, NY, announced an expansion of its services for Indian-origin families, adding specialists in marriage counseling, adult mental health, child and adolescent therapy, and family counseling.4 The platform employs clinical psychologists, licensed mental health counselors, relationship therapists, and expressive arts practitioners, and it offers therapy in English and multiple Indian languages depending on therapist availability. Notably, LeapHope does not use automated or AI-based matching, a deliberate choice that reflects how sensitive and relationship-dependent a cultural fit between therapist and client actually is.
That kind of platform growth is a signal. It confirms that demand from Indian-American families seeking culturally grounded mental health care outpaces what the existing provider landscape can currently supply.
What Most Resources Miss
A search for guidance on Indian-American couples therapy typically surfaces articles that mention cultural sensitivity in passing but stop short of clinical specificity. They rarely address arranged versus love marriage dynamics, the role of in-laws as a structural feature of the relationship rather than an external stressor, or how communication norms rooted in hierarchy and indirect speech affect the therapy room. Communication issues in couples therapy take on a distinct shape inside South Asian cultural contexts, and generic frameworks seldom account for that. This guide is designed to close that gap, offering MFTs and couples the concrete, culturally grounded framework they actually need.
Core Cultural Values That Shape Indian-American Marriages
The growing recognition that mainstream couples therapy models often fail Indian-American clients has sparked a push for frameworks that center collectivist family systems over Western individualism.
The Collectivist-Individualist Divide
In Indian-American households, marriage is rarely just a partnership between two people, it is a union of families, lineages, and extended networks. This collectivist orientation can clash directly with the individualistic assumptions baked into many therapy models. Where a standard couples session might ask, "What do you each need from this marriage?" a culturally attuned therapist reframes the question: "How do we honor the family system while addressing your personal pain?" The therapeutic frame must shift from self-fulfillment to relational interdependence, acknowledging that decisions about careers, parenting, or even weekly schedules often involve input from parents, in-laws, and siblings. Ignoring this systemic web can make the couple feel misunderstood and the therapy irrelevant. Understanding how to work with blended families in therapy and other non-nuclear structures is foundational for any MFT working in this space.
Hierarchy, Duty, and the Weight of Filial Piety
Family hierarchy is a deeply embedded norm. Elders are revered, and their opinions carry moral weight. The eldest son, in particular, often shoulders expectations to care for aging parents, manage family finances, and uphold religious or cultural traditions. For a daughter-in-law, the pressure to conform to in-law expectations around cooking, child-rearing, or participation in rituals can feel suffocating. A spouse caught between a partner and parents may present with anxiety, resentment, or emotional withdrawal. Therapists unfamiliar with these dynamics might label the conflict as poor boundaries, when in reality the system requires a nuanced negotiation of loyalty. Filial duty is not a pathology; it is a core identity thread. Setting boundaries in family therapy requires validating the moral distress while helping couples establish compassionate limits that preserve family connection without sacrificing the marital bond.
Honor, Shame, and the Stigma Barrier
In many Indian communities, the concepts of izzat (honor) and log kya kahenge (what will people say) govern behavior as powerfully as any law. Seeking therapy can feel like a public admission of failure, threatening not just individual pride but the family's social standing. This structural shame often suppresses help-seeking long after significant distress has set in. Couples may arrive in therapy only when a crisis erupts, such as infidelity, severe depression, or a threat of divorce. Infidelity couples therapy in these contexts must first address the shame narrative, normalizing therapy as a resource for strengthening, not shattering, the family name. Simple adjustments, such as assuring that sessions remain confidential even from extended family, can build essential trust.
Generational Divergence and Intra-Couple Friction
First-generation immigrants often carry these values as non-negotiable pillars of identity, while their American-born or raised children may internalize them with deep ambivalence. A second-generation Indian American woman may believe in filial piety but chafe when her husband's parents move in for six months. A first-generation husband might feel betrayed when his wife wants to celebrate holidays without the extended clan. When partners themselves come from different generational positions, one raised in India and the other in the U.S., these fault lines can open within the marriage itself. The therapist must help each partner articulate the emotional logic behind their stance, finding common ground in shared core values, perhaps reframed for a blended identity. The work is not to choose one side over the other, but to co-create a new family narrative that honors both histories.
Arranged Vs. Love Marriage Dynamics in Therapy
Most Indian-American couples seeking therapy do not fit neatly into either the "arranged marriage" or "love marriage" category that Western frameworks assume. The clinical reality is far more nuanced, and therapists who impose a binary understanding will miss critical dynamics shaping the couple's relationship.
The Spectrum of Partner Selection
Contemporary Indian-American marriages exist along a continuum that includes fully arranged unions (where families select the partner with minimal individual input), semi-arranged partnerships (family introductions followed by individual courtship and consent), and self-selected love marriages. A significant portion of second-generation Indian Americans fall into the semi-arranged middle ground, where parents facilitated initial introductions through community networks, matrimonial services, or family connections, but the couple exercised final decision-making authority.
This hybrid model has no established therapeutic framework in Western clinical training. Therapists unfamiliar with this dynamic may inadvertently pathologize family involvement or, conversely, overlook genuine autonomy violations. The therapeutic task is to explore how each partner experienced their origin story within their own cultural framework rather than measuring it against Western ideals of romantic independence.
What Research Says About Marital Satisfaction
Western assumptions often equate arranged marriages with lower satisfaction, but cross-cultural research challenges this narrative. Studies on South Asian populations have found comparable or, in some cases, higher marital satisfaction scores in arranged marriages compared to self-selected unions, particularly in samples where arranged couples reported strong family support systems and shared cultural expectations. These findings suggest that satisfaction correlates less with the method of partner selection and more with alignment of values, family integration, and communication quality. Therapists should resist the impulse to view arranged origins as inherently problematic and instead assess the specific relational patterns present in each couple.
Interfaith and Intercultural Unions
A growing subset of Indian-American couples navigates interfaith partnerships (Hindu-Muslim, Hindu-Sikh, Hindu-Christian) or intercultural marriages (Indian with non-Indian partners). These unions face distinct stressors that require targeted clinical attention. Clinicians working in this space may also find it useful to review faith-based marriage programs for marriage and family therapists, as the frameworks developed there translate meaningfully to interfaith Indian-American contexts:
Dual family systems: Each extended family may hold conflicting expectations about religious observance, holiday celebrations, and household traditions.
Religious holiday conflicts: Decisions about Diwali versus Christmas, Eid versus other observances, and which rituals to prioritize in the home can become ongoing friction points.
Child-rearing negotiations: Couples must determine how to transmit religious identity, cultural practices, and language to children when two traditions are involved.
Therapists working with these couples should map both family systems explicitly and help the couple develop protocols for managing competing demands.
Exploring the Origin Story Without Western Bias
When asking about how a couple met and decided to marry, clinicians should frame questions around the couple's own values rather than defaulting to autonomy as the highest good. Applying Bowen family systems theory can help therapists assess differentiation of self within the couple's origin story without imposing a Western hierarchy of romantic independence. Instead of asking "Did you choose your partner freely?" (which implies arranged marriages lack freedom), consider questions like:
How did your families become involved in your relationship, and what role did that involvement play?
What did commitment mean to each of you when you decided to marry?
How do you each feel about the way your partnership began, looking back now?
These questions invite reflection without imposing a hierarchy where self-selection ranks above family-facilitated partnerships. The goal is to understand how each partner experienced agency within their own cultural logic and to identify any lingering resentments or gratitudes tied to their origin story.
Questions to Ask Yourself
When you think about your marriage, whose expectations carry the most weight: your own, your partner's, or your families'?
This question surfaces a core tension in Indian-American couples therapy. Understanding where your sense of marital success originates helps identify whether conflict stems from unmet personal needs or perceived failures to meet extended family standards.
If your therapist asked you to prioritize your individual needs over family harmony, would that feel liberating or threatening?
Your gut reaction reveals how deeply collectivist values shape your relationship. A culturally competent therapist will work within your value system rather than imposing Western individualism as the default path to marital health.
Could your intake process be inadvertently signaling that arranged marriages are less healthy than love marriages?
For MFTs: Assessment questions that probe 'how you chose your partner' or assume romantic courtship can alienate couples in arranged marriages. Reviewing your forms and language for hidden bias strengthens your cultural competence from the first session.
Common Presenting Issues: In-Laws, Stigma, and Communication Styles
In-law interference ranks as the single most common presenting issue for Indian-American couples seeking therapy, often eclipsing even financial stress in intake assessments. For clinicians trained in Western models, the challenge is to distinguish between culturally normative family interdependence and patterns that genuinely undermine the marital subsystem. Boundary negotiation within structural family therapy does not look like the individuation work prized in Euro-American therapy; the therapist must validate the couple's embeddedness within the extended family while helping them carve out a private domain for their partnership.
Reframing the In-Law Dynamic: Boundaries Within Belonging
Attempting to label close in-law involvement as enmeshment can inadvertently alienate clients who view elder respect and family unity as non-negotiable values. A more effective approach reframes the issue as a boundary negotiation within the established collectivist structure. Instead of pushing for separation, the therapist helps the couple articulate where they need autonomy and where they are willing to accommodate family expectations. For example, a wife may want her mother-in-law to stop entering the kitchen unannounced, but she does not want to stop eating dinner together nightly. The clinician's task is to guide the couple in presenting these requests not as rejection but as a bid for modified, respectful collaboration.
Mental Health Stigma: From Barrier to Clinical Dynamic
Stigma around mental health in Indian communities does more than delay help-seeking; it shapes the very presentation of the couple in the therapy room. Many first- and second-generation clients minimize distress, reframe therapy as "advice-seeking" from a wise elder, or only attend when the relationship is in acute crisis. Therapists must resist interpreting these patterns as resistance or low motivation. Normalizing the stigma, openly acknowledging the courage it takes to sit in a therapist's office given community attitudes, can be a powerful joining tool. Clinicians can also frame therapy as a practical, solution-focused endeavor, aligning with cultural preferences for concrete guidance over emotional exploration. Narrative therapy techniques offer another entry point here, using a client's own storytelling traditions to externalize stigma rather than personalize it.
Communication Styles: Silence, Indirectness, and Conflict Avoidance
Communication patterns that might be pathologized in mainstream contexts are often normative and functional in Indian families. Indirect communication, use of third parties to relay sensitive messages, and long pauses in conversation are common and can reflect respect, thoughtfulness, or a wish to preserve harmony. A therapist must learn to differentiate cultural communication from clinical avoidance. For instance, a husband's silence during a session may indicate deference, not stonewalling. Key culturally informed communication features to assess include:
Indirect refusal: Saying "I'll try" instead of "no" to avoid confrontation.
Triangulation: Relying on a family elder to mediate disputes.
Storytelling: Using parables or examples from others to express personal feelings.
Code-switching: Shifts between English and an Indian language when emotionally activated.
Generational Differences in Presenting Concerns
First-generation immigrant couples typically bring issues rooted in migration stress, role renegotiation, and acculturative gaps with children. A wife who becomes the primary breadwinner for the first time may clash with a husband socialized to be the provider. Second-generation couples, born or raised in the U.S., more often present with identity conflicts, parental pressure around career or partner choice, and the emotional fallout from defying family expectations in love marriage situations. Recognizing these generational patterns helps the therapist target interventions: skills-building and psychoeducation for first-gen couples, versus identity exploration and differentiation work for second-gen partners. Marriage and family therapy modalities that blend systemic and narrative approaches tend to serve both generational profiles more flexibly than single-model treatments.
Adapting EFT, Gottman, and CBT for Indian-American Collectivist Family Structures
The evidence base for couples therapy has grown considerably over the past two decades, yet most of that research was built on samples that look nothing like Indian-American families.
What the Research Actually Shows
As of 2026, no randomized controlled trial has tested a culturally adapted version of Emotionally Focused Therapy (EFT), the Gottman Method therapy, or Cognitive Behavioral Therapy (CBT) specifically with South Asian or Indian-American couples.1 That gap is real, and therapists working with this population should know it exists rather than assume mainstream protocols transfer without adjustment.
That said, the available research is not empty. A 2017 pilot study using a Systemic-Constructivist Couple Therapy (SCCT) model with South Asian Canadian couples found significant improvement in relationship adjustment after the intervention.2 The mechanism appeared to be a strengthening of what researchers called "couple identity," meaning the partners' shared sense of themselves as a unit, which can be complicated in collectivist families where individual and couple identity are subordinate to the extended family system. The study used a single-group pre-post design with no comparison arm, so the findings are promising rather than conclusive, but they represent the most direct couple-level evidence available.
Broader meta-analytic work published in 2006 found that culturally adapted mental health treatments consistently outperform non-adapted treatments for ethnic minority clients.3 More recent systematic reviews of culturally adapted CBT for South Asian populations confirm this pattern, with adaptations centered on family involvement, language accessibility, and the integration of spiritual or religious values producing better outcomes than standard protocols.4
Where the Knowledge Gap Sits
A 2020 review from Oxford University Press noted plainly that relatively little is known about how to adapt established couple therapy models for racially and ethnically diverse families.5 A 2022 systematic review found an absence of published articles specifically focused on culturally adaptive approaches for South Asian clients in couples or family contexts.6 Guidelines for working with Asian Indian American couples were proposed as early as 2012, but those frameworks have not yet been put through empirical testing.7
For therapists, this means clinical judgment and cultural humility carry more weight than a protocol manual. Adapting EFT for an Indian-American couple might mean acknowledging that attachment styles were shaped not just by early caregiving but by multigenerational family loyalty, a dynamic well-illuminated by Bowen family systems theory. Applying Gottman-based communication tools requires sensitivity to the fact that direct conflict expression may carry social consequences outside the therapy room. CBT thought records may need to account for collective cognitions, not just individual automatic thoughts.
How to Stay Current
Because peer-reviewed studies on this topic remain sparse, therapists and MFT doctoral program graduates looking to build competence should draw from multiple sources:
Academic databases: Search APA PsycNet, the Journal of Marital and Family Therapy, and PubMed using terms like "culturally adapted couples therapy South Asian" to catch new studies as they are published.
Dissertation research: ProQuest holds graduate theses on Indian-American couples therapy that include cultural adaptation frameworks not yet published in journals.
Professional associations: APA Division 43 (Couples and Family Therapy) and the South Asian Mental Health Initiative and Network (SAMHIN) publish reports, webinars, and research summaries that bridge the gap between academic publication cycles and clinical practice.
University family therapy programs: Faculty at programs with a cultural adaptation focus may have unpublished or ongoing research relevant to South Asian couples work that is not yet indexed anywhere.
The honest clinical picture is this: the general finding that cultural adaptation improves outcomes is well-supported. The specific application to Indian-American couples therapy is still being built. Practitioners who engage with that uncertainty directly, rather than importing untested assumptions from mainstream models, are likely to serve this population far better.
Cultural competence in couples therapy is not about memorizing Indian customs. It is about knowing when a Western framework's default assumptions (autonomy is healthy, enmeshment is pathological, direct communication is superior) will alienate the couple before therapy even begins. Therapists who fail to interrogate these assumptions risk imposing a model of marriage that conflicts with the couple's values, undermining trust and progress from the first session.
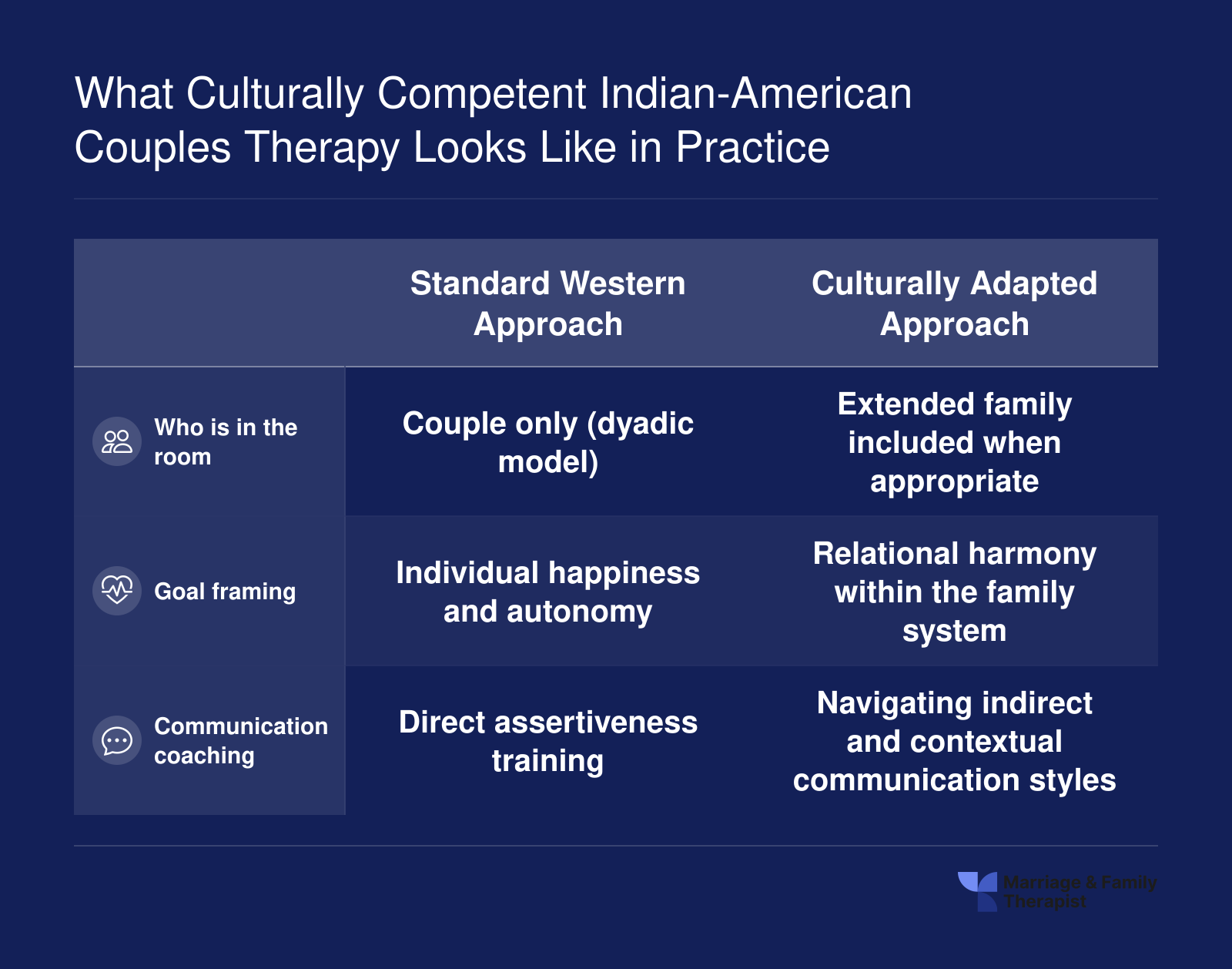
What Culturally Competent Indian-American Couples Therapy Looks Like in Practice
Culturally competent therapy does not simply translate Western techniques into another language. It reframes the entire therapeutic lens to honor collectivist values, family structures, and communication norms that shape Indian-American marriages. Here is how a culturally adapted approach differs across three critical dimensions.
How to Find a Culturally Competent Indian-American Marriage Therapist
Finding the right therapist is one of the most consequential steps an Indian-American couple can take. A clinician who understands collectivist family dynamics, immigration stress, and the role of spirituality in daily life will be far more effective than one who treats every couple through a Western individualist lens. The good news: several directories and platforms now make this search easier than it was even a few years ago.
Competencies to Look For
Before you start browsing directories, know what you need. Use the checklist below to evaluate any therapist you are considering.
Language access: Can the therapist conduct sessions in Hindi, Gujarati, Tamil, Urdu, Punjabi, Bengali, or another language you and your partner are most comfortable expressing emotions in? Even couples fluent in English often find that switching to a home language unlocks deeper vulnerability.
Collectivist family systems experience: Has the clinician worked with families where parents, in-laws, and extended kin are active participants in marital decisions? Specializing in family systems therapy equips clinicians to navigate exactly these layered relational structures.
Arranged and semi-arranged marriage familiarity: Does the therapist understand the spectrum from fully arranged to love marriages, and avoid pathologizing either end?
Immigration and acculturation awareness: Can they address visa-related stress, cultural code-switching, and the grief of living far from family?
Religious and spiritual comfort: Will they respectfully incorporate Hindu, Sikh, Muslim, Jain, Christian, or other faith frameworks when those frameworks matter to you?
Where to Search
Several platforms cater specifically to South Asian or Indian-origin communities.
LeapHope is a Brooklyn-based online therapy platform founded by Shwati Singh that focuses on Indian diaspora and NRI couples.1 Its network includes U.S.-licensed professionals and RCI-registered Indian psychologists, with sessions available in English, Hindi, and Arabic.2 LeapHope does not use automated or AI-based therapist matching, relying instead on human curation. As of mid-2026, the platform serves clients across 16 countries, including the United States, Canada, the UK, Australia, the UAE, and India.1
SAAADA (South Asian Americans Against Domestic Abuse) maintains referral lists that can help couples find therapists experienced with South Asian relational dynamics, particularly when power imbalances or abuse are concerns.
Psychology Today's therapist directory lets you filter by ethnicity, language, and specialty. Search for "South Asian" or a specific language, then narrow by "couples therapy" or "family systems."
AAMFT Therapist Locator from the American Association for Marriage and Family Therapy connects you with credentialed LMFTs. While it does not have a South Asian filter, you can review individual profiles for cultural competence indicators.
South Asian Mental Health (SAHM) resources aggregate clinicians and support groups specifically for South Asian communities.
Keep in mind that under current U.S. telehealth law, therapy is considered to take place in the state where the client is located,3 so confirm that any teletherapy platform for marriage and family therapists you consider is staffed by clinicians licensed in your state.
Questions to Ask During a Consultation Call
Most therapists offer a brief introductory call. Use it wisely. Consider asking:
"Have you worked with Indian-American couples before, and what did those cases typically involve?"
"How do you handle in-law dynamics when they are a central source of conflict?"
"Would you be willing to include family members in sessions if we request that?"
"How familiar are you with the stressors that come with immigration or living far from extended family?"
"Are you comfortable discussing religious or spiritual practices as part of treatment?"
A therapist who answers these questions with specificity, rather than vague assurances, is far more likely to deliver meaningful care.
Ethnic Matching Is Preferred but Not Required
Research suggests that ethnic matching can strengthen the therapeutic alliance, particularly when shame or stigma is involved. However, a non-South Asian therapist who has completed genuine cultural competence training, supervised work with collectivist families, or continuing education focused on South Asian communities can be highly effective. What matters most is that the clinician demonstrates curiosity, humility, and a willingness to learn about your world rather than assuming they already understand it. If you connect well during the consultation call and the therapist checks most of the boxes above, their ethnic background alone should not be a disqualifier.
Insurance, Costs, and Access to Culturally Competent Care
Couples therapy in the United States runs $150 to $300 per session nationally in 2025-20261, and climbs to $250 to $600 in major metro areas like the Bay Area, New York, and Washington D.C., where much of the Indian-American population is concentrated. For Indian-American couples seeking a therapist who speaks Hindi, Tamil, Gujarati, Punjabi, or Bengali, or who understands joint-family dynamics without a lengthy explanation, the sticker price is often only the beginning of the affordability conversation.
How Insurance Actually Covers Couples Work
Most major insurers (including Aetna, Cigna, United, and Blue Cross plans) will only cover couples therapy when one partner carries a diagnosable mental health condition and the treatment plan is documented as medically necessary.2 The therapist typically bills CPT code 90847 (family psychotherapy with the patient present), or 90834 and 90837 for individual sessions.3 If the presenting problem is framed purely as "marital conflict" without an underlying diagnosis such as an adjustment disorder, generalized anxiety, or major depression, the claim is usually denied.4 ACA plans must cover behavioral health as an essential health benefit, but that mandate does not extend to purely relational concerns. Medicare Part B covers 80% of medically necessary outpatient psychotherapy after the deductible, though the pandemic-era telehealth flexibilities are set to expire September 30, 2025 unless Congress extends them.6
When therapy is covered, insured copays typically land at $30 to $50 per session.7 There are no special billing codes or enhanced reimbursement for culturally specific or multilingual care8, a structural gap that quietly limits supply.
Out-of-Network Strategies and the Access Gap
Culturally competent, multilingual South Asian therapists are disproportionately out-of-network, in part because in-network reimbursement rates rarely reflect the specialized training and language skills involved. PPO plans usually reimburse 50% to 70% of the allowed amount after a separate out-of-network deductible.9 Practical workarounds:
Superbills: Ask your therapist for a monthly superbill you submit to your insurer for partial reimbursement.
HSA and FSA accounts: Therapy is an eligible expense, effectively giving you a 22% to 37% discount depending on your tax bracket.
Reimbursement platforms: Services like Reimbursify and Thrizer file out-of-network claims on your behalf.
Sliding scale: Many South Asian therapist collectives offer $30 to $80 sessions based on income.1
Online private-pay care typically runs $260 to $480 per month, versus $600 to $1,200 for weekly in-person sessions.1 Telehealth is the geographic equalizer here: a couple in suburban Ohio can now work with a Marathi-speaking LMFT in New Jersey. Therapists exploring this space may find it useful to review how to start an online couples therapy practice before accepting cross-state clients. Platforms like LeapHope, the Brooklyn-based service that expanded its Indian-origin family network on July 16, 2026, illustrate this shift, matching couples with human clinicians (not algorithms) across English and multiple Indian languages regardless of ZIP code. For clinicians on the business side, financial therapy represents a related niche worth considering for clients navigating the cost burdens that often accompany cross-cultural family stress.
Asian American adults access mental health treatment at about half the rate of the general U.S. population: 12.5% compared to 22.7% nationally, according to SAMHSA's 2024 National Survey on Drug Use and Health. This gap underscores the urgent need for culturally responsive MFTs who understand the stigma, family dynamics, and access barriers facing South Asian and Indian-American communities.
Building Cultural Competence: What MFT Programs and LMFTs Should Know
What specific training do MFT programs and practicing therapists need to serve Indian-American couples effectively, and where can they get it?
The answer begins with accreditation standards and extends into coursework, continuing education, and language skills that make a measurable difference in clinical outcomes.
COAMFTE Standards Now Require Cultural Competence Training
The Commission on Accreditation for Marriage and Family Therapy Education (COAMFTE) sets the bar for MFT graduate programs across the country. Its accreditation standards include 10 foundational curriculum areas, and among them is a clear mandate: programs must address diverse, multicultural, and underserved communities.1 Cultural humility is also a required competency, not an elective add-on.2 These standards mean that every COAMFTE-accredited online MFT programs| graduating new LMFTs is expected to prepare clinicians who can work across cultural lines, including with Indian-American and South Asian families.
For prospective MFT students, this requirement creates a useful filter. Programs that go beyond the minimum standard and embed multicultural coursework deeply into their curricula are better positioned to prepare you for the realities of practice with collectivist family systems.
Programs With Strong Multicultural Curricula
Several COAMFTE-accredited programs stand out for the depth of their multicultural training:
Northwestern University: Examines race, culture, gender, sexuality, religion, and other aspects of identity within its MFT curriculum, with an explicit emphasis on cultural humility.3
University of Louisville: Trains culturally responsive couple and family therapists with a strong social justice orientation.
Mercer University: Offers specialized training in diversity, gender, and racial issues alongside social justice frameworks.
Syracuse University: Integrates cultural humility and social justice throughout its MFT coursework.
Alliant International University: Focuses on developing culturally competent therapists prepared for diverse populations.
Capella University: Aims to prepare graduates who can foster culturally and ethnically sensitive academic and community environments.1
UMass Global, Texas Wesleyan University, Southern Connecticut State University, and Abilene Christian University: Each incorporates cultural competence or cultural humility as core program goals.
Continuing Education for Practicing LMFTs
Licensed therapists who completed their degrees before multicultural coursework was standard still need pathways to build these skills. Options include:
Cultural humility workshops: Organizations such as the South Asian Mental Health Initiative and Network (SAMHIN) and the Asian Mental Health Collective offer trainings that address stigma, family dynamics, and culturally specific presenting issues.
Supervised clinical hours with diverse populations: Seeking practicum placements or post-licensure supervision in community settings that serve immigrant and South Asian families helps translate theoretical knowledge into clinical skill. See MFT clinical internship guidance for what to expect when seeking diverse placements.
AAMFT-approved continuing education: The American Association for Marriage and Family Therapy lists CE courses that cover multicultural practice, and many state licensing boards accept these credits toward renewal. Checking LMFT continuing education requirements by state can help you confirm what counts toward your specific renewal cycle.
The goal is not a single workshop but sustained engagement with the communities you intend to serve.
Language as a Clinical Asset
The ability to conduct therapy in Hindi, Gujarati, Tamil, Urdu, or other Indian languages is more than a convenience. It can unlock emotional expression that clients struggle to access in English, particularly around topics like family obligation, shame, or spiritual distress. LeapHope, a Brooklyn-based online mental health platform that expanded its services in July 2026, offers therapy in English and multiple Indian languages depending on therapist availability.6 The platform's multilingual model reflects real market demand: Indian-origin families actively seek therapists who can meet them in their primary language.
For MFT students and early-career LMFTs, investing in therapeutic vocabulary in one or more South Asian languages can distinguish your practice and open doors to an underserved client population. Even basic conversational proficiency signals cultural investment that builds trust in the therapeutic relationship.
Frequently Asked Questions About Indian-American Couples Therapy
Indian-American couples often have specific questions before starting therapy, especially when cultural dynamics play a central role in their relationship. Below are answers to the most common concerns, grounded in what the clinical literature and professional guidelines currently support.
What makes a therapist culturally competent for Indian-American couples?
A culturally competent therapist understands the values that shape Indian-American family life, including collectivism, respect for elders, family hierarchy, and the significance of community reputation. Beyond awareness, the therapist actively integrates these factors into treatment planning rather than applying a one-size-fits-all Western framework. Professional organizations such as the American Association for Marriage and Family Therapy (AAMFT) and the American Psychological Association (APA) publish practice guidelines emphasizing the importance of cultural humility, ongoing self-education, and responsiveness to each client's unique cultural context. Understanding LMFT vs. marriage counselor distinctions can also help couples choose the right credential when searching for a provider.
Are outcomes better when the therapist shares the couple's ethnic or cultural background?
Research on ethnic and cultural matching in therapy is still evolving, particularly for South Asian and Indian-American populations. Peer-reviewed databases such as PsycINFO, PubMed, and Google Scholar contain a growing body of work under keywords like "therapist ethnic matching," "South Asian couples therapy," and "Asian American cultural matching outcomes." Some meta-analyses and systematic reviews published in journals such as the Annual Review of Clinical Psychology and Clinical Psychology Review suggest that cultural matching can strengthen the therapeutic alliance, but the evidence is not uniform across all populations. A therapist who does not share the couple's background but has deep training in South Asian cultural dynamics can also achieve strong outcomes. The most consistent finding is that cultural responsiveness, not ethnicity alone, predicts client satisfaction and progress. Research on MFT clinical effectiveness over time reinforces that responsiveness and deliberate practice matter more than any single therapist characteristic.
How do therapists handle conflicts between American individualism and Indian family obligations?
This is one of the most common presenting issues in Indian-American couples therapy. A skilled therapist helps couples identify where Western values around personal autonomy and Indian values around familial duty create friction, then works with the couple to negotiate boundaries that honor both partners' needs. Rather than framing one value system as superior, culturally competent clinicians treat the tension itself as a normal part of bicultural life and help couples develop shared language for discussing it.
Where can I find peer-reviewed research on culturally adapted therapy for Indian-American couples?
Start with PsycINFO or PubMed using search terms like "South Asian couples therapy" or "culturally adapted marriage counseling." The Journal of Multicultural Counseling and Development frequently publishes relevant studies. University counseling and psychology departments with Asian American mental health research programs can also be valuable resources; some maintain databases of published and in-progress studies. For broader context, look for systematic reviews in the Clinical Psychology Review that summarize evidence on cultural adaptation of evidence-based treatments.
How much does culturally competent couples therapy typically cost?
Session fees vary widely depending on location, therapist credentials, and whether the practice is in-person or online. In general, couples therapy rates in the United States range from moderate to high per session, with licensed marriage and family therapists vs. clinical psychologists each setting their own fee structures. Some culturally focused platforms and group practices offer sliding-scale fees. Insurance coverage also varies by plan and state; it is worth verifying whether your insurer covers couples therapy and whether in-network providers with cultural competence in South Asian family dynamics are available.
Can therapy be conducted in Hindi, Gujarati, Tamil, or other Indian languages?
A growing number of therapists in the U.S. offer sessions in Indian languages, though availability depends on your region and the specific language you need. Online platforms have expanded access considerably. For example, LeapHope, a Brooklyn-based online mental health platform founded by Shwati Singh, announced in July 2026 that it expanded its network to include specialists in marriage counseling, family counseling, and other areas, with therapy available in English and multiple Indian languages depending on therapist availability.1 Directories on marriagefamilytherapist.org and professional association databases can also help you filter by language when searching for a provider.