Addressing Life-Stage Conflicts: Fertility, Finances, and Caregiving
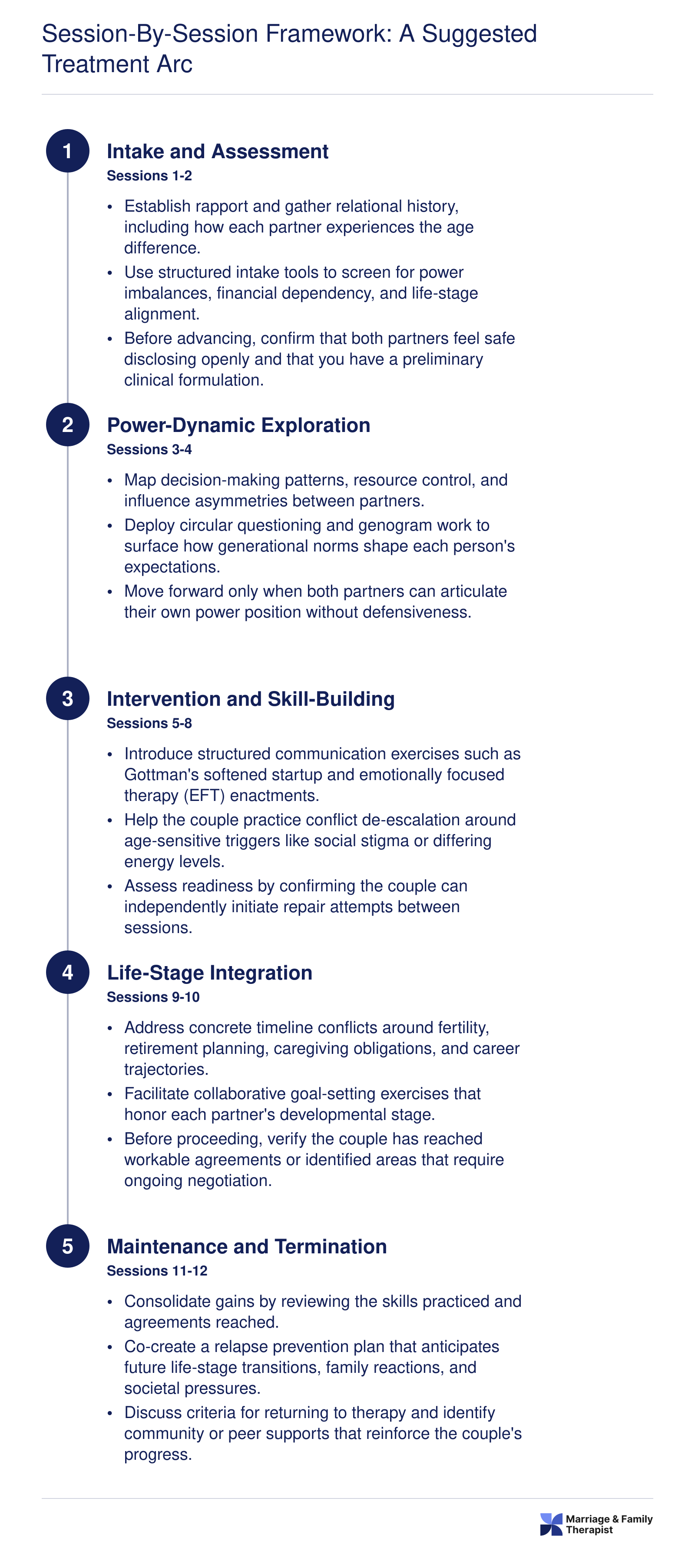
Three timeline mismatches surface more than any others in age-gap couples therapy: fertility windows, retirement-versus-career-peak financial planning, and eldercare obligations that fall disproportionately on the younger partner. Each of these domains carries both logistical weight and deep emotional significance, and MFTs who treat them as scheduling problems alone risk missing the attachment injuries they conceal.
Fertility, Financial Planning, and Caregiving as Clinical Priorities
Fertility conflicts often emerge when one partner has already passed their reproductive window or has no interest in additional children while the other envisions parenthood as a core life goal. The conversation is rarely just about biology. It touches identity, legacy, and the question of whether each partner feels fully seen by the other. MFTs working in this space may find that pre-conception couples therapy frameworks offer a useful foundation for structuring these early fertility conversations.
Financial planning creates a parallel tension. One partner may be approaching retirement and shifting into wealth preservation mode while the other is at a career peak, investing aggressively, and envisioning decades of earning ahead. Assumptions about shared accounts, lifestyle expectations, and estate planning can go unspoken for years until a triggering event, such as a job loss or health scare, forces them into the open.
Caregiving obligations round out this triad. Younger partners frequently absorb eldercare duties for the older partner's parents or, eventually, for the older partner themselves. Without explicit discussion, this can breed resentment that erodes the relationship from within.
The Parallel Timeline Exercise
A practical in-session tool for surfacing these mismatches is the Parallel Timeline technique. Each partner independently maps their anticipated next ten to twenty years on a large sheet of paper or whiteboard, marking milestones such as desired career transitions, health concerns, family goals, and financial benchmarks. The therapist then places these timelines side by side and facilitates a joint review, highlighting overlaps and gaps.
This exercise works because it externalizes assumptions. Partners often discover that they have never voiced key expectations, not out of secrecy, but because they assumed alignment. Seeing a gap on paper, such as one partner planning to relocate at sixty while the other expects to be launching a business at forty, transforms an abstract worry into a concrete discussion point.
Therapeutic Questions That Unlock Unspoken Assumptions
MFTs can deepen the Parallel Timeline conversation with targeted prompts:
- "What does your ideal life look like at fifty-five? At seventy? Walk me through a typical week in that future."
- "If your partner's timeline for this milestone differs from yours by five or more years, what feelings come up for you right now?"
- "Whose needs do you imagine will take priority in the next decade, and how does that expectation sit with you?"
These questions are designed to move the couple past logistics and into affect. When a partner realizes they have been silently grieving a parenthood timeline that no longer seems possible, or quietly resenting an anticipated caregiving role they never agreed to, the therapist can reframe the moment as an attachment-relevant disclosure rather than a scheduling conflict.
Reframing Logistics as Attachment Work
Clinicians should expect that Parallel Timeline conversations will surface latent grief or resentment. A younger partner who discovers they may spend their forties caring for an aging spouse is not just facing a calendar problem. They are confronting questions about reciprocity, sacrifice, and whether the relationship can hold the weight of that imbalance. Similarly, an older partner who learns that their spouse privately mourns the children they will not have together may experience shame or guilt that predates the relationship itself.
By naming these emotions and linking them to attachment needs, such as the need to feel chosen, valued, and secure in a shared future, MFTs elevate what could be a transactional negotiation into meaningful therapeutic work. Emotionally focused therapy offers a particularly well-suited framework for this kind of attachment-oriented reframing. The goal is not to resolve every mismatch in a single session but to establish a pattern of transparent, emotionally honest dialogue that the couple can sustain beyond the therapy room.