Structural and Systemic Models: Understanding Boundary Problems in Families
Structural family therapy and Bowenian theory continue to offer the most precise vocabulary for understanding why some families treat therapy as permission to air every grievance while others can barely share a feeling. Recognizing these patterns requires familiarity with the models that define healthy and problematic boundaries.
Structural Family Therapy: Three Boundary Types
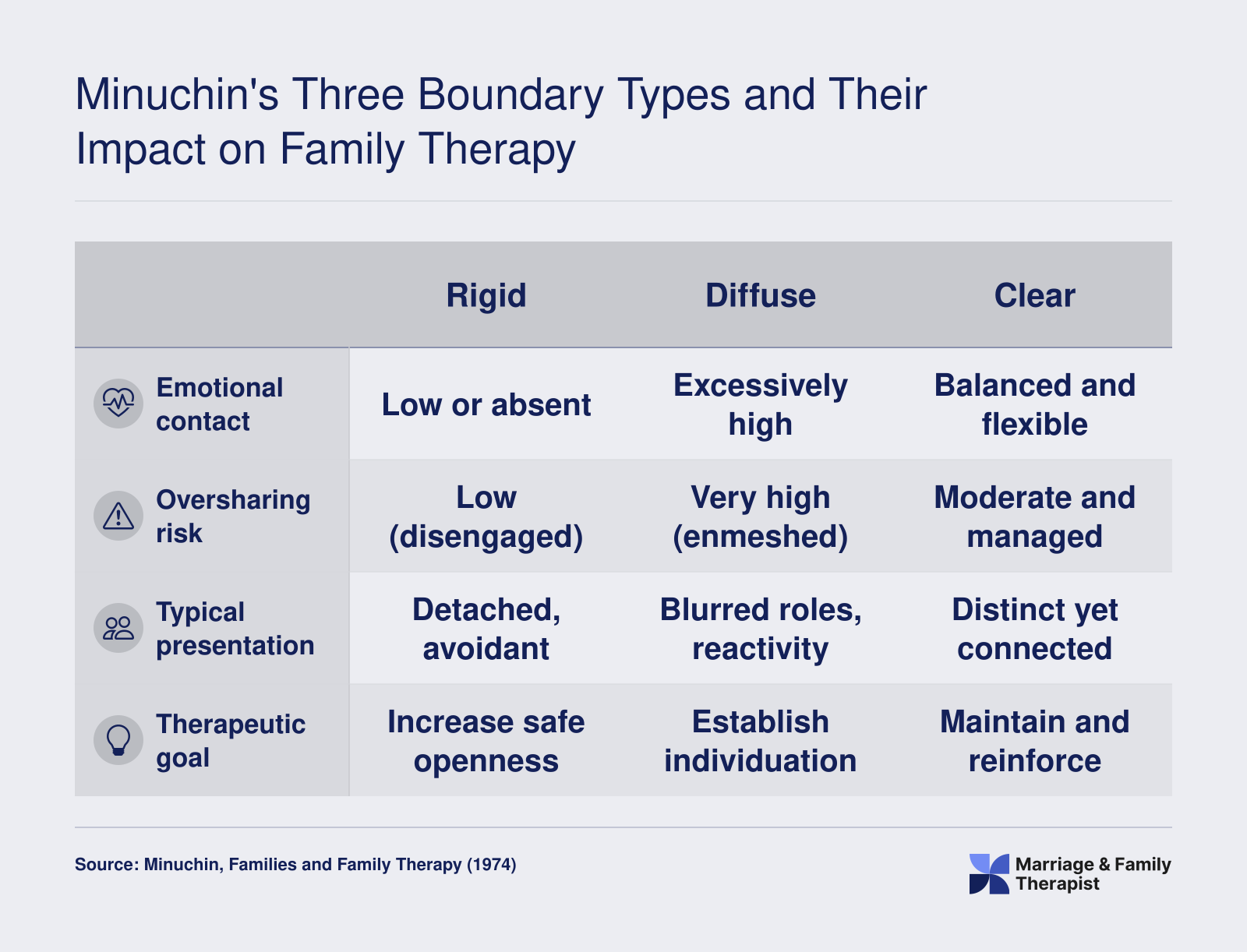
Structural family therapy, developed by Salvador Minuchin, categorizes family boundaries along a continuum: clear, rigid, and diffuse. Clear boundaries allow age-appropriate autonomy while preserving emotional connection, and members share selectively and respect individual privacy. Rigid boundaries produce disengaged families where emotional distance is the norm; here, oversharing may erupt abruptly as a desperate attempt to bridge long-standing disconnection, catching the therapist off guard. Diffuse boundaries, by contrast, define enmeshed families where members routinely share too much too soon, assuming everyone is entitled to every thought and feeling. In these systems, oversharing is not a therapeutic error but a reflection of the family's operating rules.
Enmeshment Versus Healthy Closeness
The distinction between enmeshment and healthy closeness is critical. Enmeshed families exhibit blurred roles, emotional contagion, and a loss of individual identity. A child may speak for a parent, or a spouse may disclose intimate details that belong in a private diary. Healthy closeness, however, maintains differentiation: members remain warmly connected yet can think, feel, and speak as separate individuals. Therapists assess this by noting who interrupts, who assumes consent to share another's story, and how easily one member becomes dysregulated by another's emotion. When enmeshment drives oversharing, the therapist's task shifts from simple redirection to restructuring the family's boundary rules.
Differentiation of Self and Emotional Reactivity
Bowen family systems theory explains why some family members cannot regulate their disclosures through the concept of differentiation of self. Lower differentiation correlates with emotional fusion: individuals react impulsively to relationship anxiety by flooding the session with intense, unprocessed material. They may reveal painful secrets not to resolve them but to relieve internal pressure or to enlist the therapist as an ally. A highly differentiated person, by contrast, can reflect before speaking and tolerate the discomfort of withholding information until it serves a therapeutic purpose. Training therapists to spot low differentiation helps them anticipate boundary violations and intervene with psychoeducation about self-regulation before dialogue escalates.
Validated Tools for Assessing Family Boundaries
Clinicians have several empirically validated instruments to evaluate boundary functioning. The FACES IV assessment (Olson, Gorall, & Tiesel, 2011) is a 42-item measure using a 5-point Likert scale that evaluates cohesion and flexibility across balanced and unbalanced subscales, including Enmeshed and Disengaged dimensions.1 Internal consistency coefficients from the 2011 validation study are strong across subscales: Balanced Cohesion (.89), Balanced Flexibility (.84), Disengaged (.87), Enmeshed (.77), Rigid (.82), and Chaotic (.86).2 The Boundary Ambiguity Scale, developed by Pauline Boss, assesses confusion about family membership and role clarity, a factor closely linked to inappropriate self-disclosure.3 Additionally, the Family Communication Scale and Family Satisfaction Scale, both developed by Olson, offer insight into how communication patterns and relational contentment influence boundary maintenance.4 These tools allow therapists to move beyond intuition and map the specific structural dysfunctions that fuel oversharing.
From Theory to Intervention: Reframing Oversharing as Systemic Pattern
When a therapist identifies diffuse boundaries in session, the oversharing is no longer just a behavior to stop; it becomes a systemic pattern to address. The intervention may begin with a structural observation: "I notice that everyone here feels responsible for holding everyone else's feelings. I wonder if we can practice letting each person speak for themselves." This reframe shifts the conversation from blaming an individual to reorganizing the family's rules for privacy and respect. Similarly, when rigid boundaries underlie sporadic oversharing, the goal becomes building gradual, predictable pathways for disclosure that feel safe rather than explosive. Theory equips the therapist to see oversharing as a symptom of the family's organization, and to design interventions that reshape that organization rather than merely suppress the symptom.