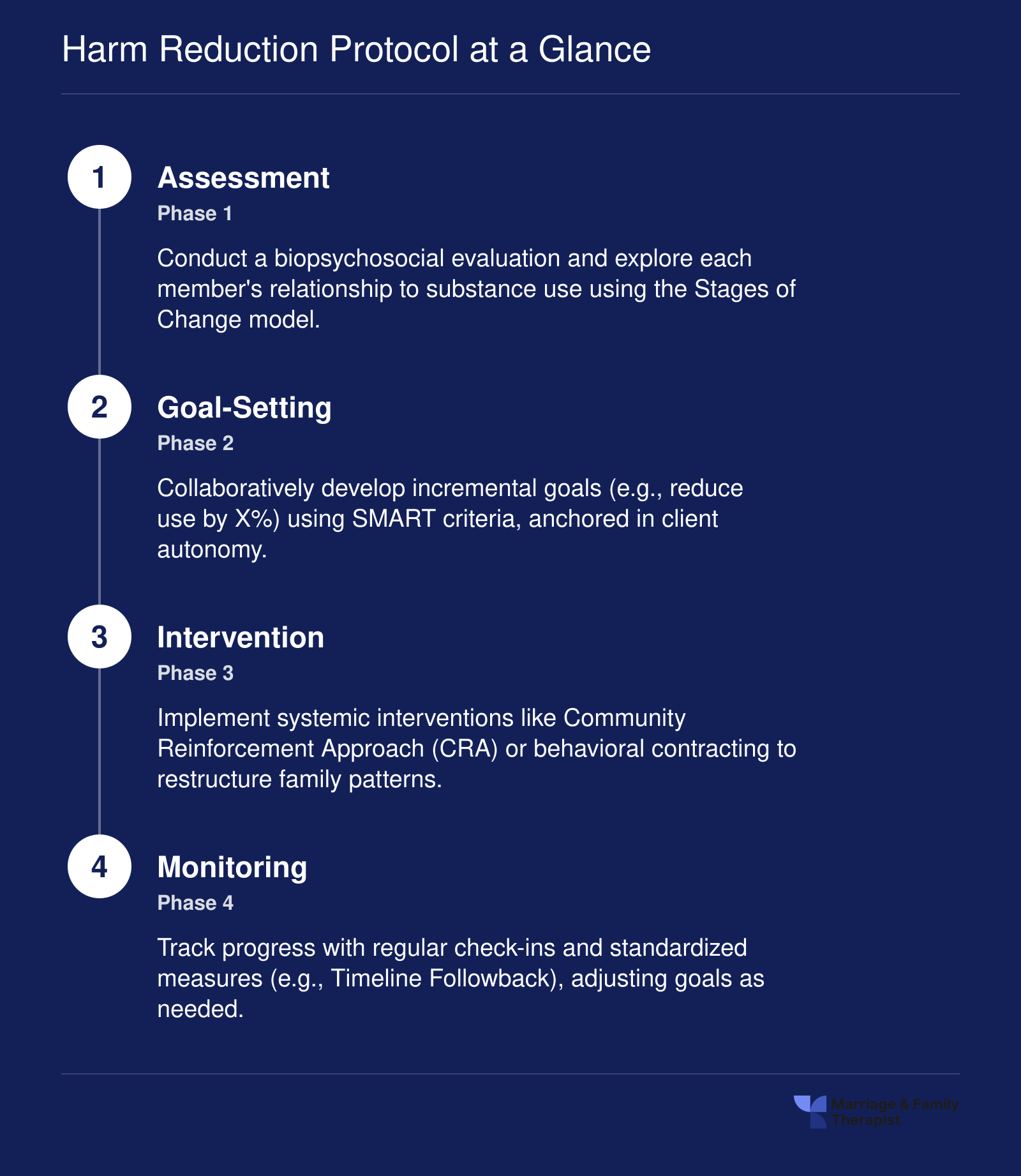
Ethical Dilemmas, Risk Management, and Child Safety in Harm Reduction Family Work
Embracing harm reduction in family therapy does not mean abandoning ethical safeguards. In fact, working within a non-abstinence framework demands heightened vigilance around informed consent, documentation, and risk assessment to protect both clients and the therapist's license. The AAMFT Code of Ethics provides clear guidance on competence, confidentiality, and duty to warn that directly apply to harm reduction practice, but state licensing boards and mandatory reporting laws add layers of complexity, especially when children are involved.1
Ethical Pressure Points: Five Areas of Concern
Five ethical challenges surface repeatedly in harm reduction family work. First, informed consent for a harm reduction frame must be explicit and ongoing. The AAMFT Code requires marriage and family therapists to disclose the risks and benefits of any treatment approach, including emerging or non-traditional models like harm reduction (see Standards 3.11 on professional competence and 1.11 on non-abandonment).1 Clients must understand that the goal is not necessarily abstinence, but safer substance use patterns and relational health, and that they can revisit the treatment plan at any time.
Second, intimate partner violence (IPV) screening becomes critical when substance use is present. The intersection of coercion, control, and intoxication can escalate risk, so therapists must routinely assess for IPV and have a safety plan that acknowledges substance-related dynamics.
Third, child safety and mandatory reporting create the most acute ethical tension. Reasonable suspicion of child abuse or neglect compels reporting, but the threshold can be ambiguous in harm reduction cases.1 Standard 7.7 of the AAMFT Code addresses custody and treatment of minors, emphasizing the child's best interest, while Standard 6.3 governs confidentiality exceptions. Simply having a parent who uses substances does not automatically constitute neglect; only when use directly endangers the child (e.g., driving while impaired, unsafe storage, leaving children unattended) does the duty to report typically activate.
Fourth, duty to warn or protect applies when a client poses a serious risk of harm to an identifiable third party. In family therapy, this might arise if a family member's substance use directly threatens another's physical safety.3 The AAMFT's guidance on dangerous patients and termination reinforces that therapists must assess severity and act proportionately.
Fifth, documentation standards become more rigorous under a harm reduction model.3 Therapists must document not only clinical progress but also the ongoing risk-benefit analysis and the justification for a non-abstinence goal. Clear notes serve as both a clinical roadmap and a legal safeguard.
Managing Liability: Does a Non-Abstinence Goal Create Risk?
A common malpractice concern is whether endorsing a non-abstinence goal creates liability if a client later causes harm. The short answer is no, provided the therapist has practiced within standard of care. Harm reduction is a recognized and ethically permitted approach, as confirmed by AAMFT discussions and AAMFT Legal and Ethics Fact Sheets from 2020 to 2026.4 Liability arises from negligence, not from the goal itself.
Thorough informed consent is the linchpin of risk management. A practical documentation concept for a client whose stated goal is reduced use rather than abstinence would include:
- The specific harm reduction goal (e.g., client will reduce opioid use by 50% over three months) and its rationale.
- A discussion of potential risks (escalation of use, relationship strain, child protective services involvement) and benefits (preserving trust, avoiding disengagement).
- An explicit statement that the client understands alternatives, including abstinence-based treatment, and chooses this course.
- A signed informed consent addendum that is regularly revisited.
Such documentation demonstrates shared decision-making and shields against claims of abandonment or incompetence.
A Tiered Child-Safety Framework in Harm Reduction Family Work
Child safety monitoring must be continuous and calibrated to the level of risk.4 A practical three-tier model helps therapists intervene appropriately:
- Low risk: The parent shows stable reduction or consistent use patterns that do not impair caregiving (e.g., using only after children are asleep, no drug paraphernalia accessible). The home environment remains safe, and the child is not exposed to substance-related harm. In these cases, ongoing monitoring and support may be sufficient, with clear boundaries about when reporting would be triggered.
- Moderate risk: Use patterns are inconsistent, or the child is in the home when substances are present but there is no immediate neglect. For example, a parent occasionally becomes intoxicated while the other parent provides care. Here, therapists should intensify safety planning, perhaps requiring a designated sober caregiver at all times and using a lockbox for substances, and document the elevated risk closely. CPS consultation without identifying information may be advisable to clarify reporting thresholds.
- High risk: Active impairment during caregiving, unsafe storage of substances (e.g., needles or pills within reach), or evidence of neglect or abuse. Mandatory reporting is likely required, but the therapist should first attempt to engage the family in a voluntary safety plan while abiding by legal obligations. Involving CPS can sometimes be done collaboratively, framing it as a support rather than a punitive action.
Concrete Safety-Planning Interventions
Therapists working within a harm reduction frame must equip families with practical tools. Key interventions include:
- Designated sober caregiver agreements: Families identify at least one adult who will remain unimpaired during specific windows when children need supervision. This may involve shift parenting or reliance on extended family.
- Substance lockbox protocols: Clients agree to store all substances in a locked container separate from living areas, with access restricted to the person using and under agreed conditions.
- Escalation plans: A written, step-by-step plan for what happens if the parent's use increases to the point of impairment during caregiving. This might include an immediate call to a sober support person or, in extreme cases, a temporary voluntary placement of children with a trusted relative.
These plans should be documented and signed by all adults in the therapeutic system to reinforce commitment and shared responsibility.
Cultural and Intersectional Considerations
Harm reduction family therapists cannot ignore the disproportionate involvement of child protective services with families of color. Mandated reporting, while legally required, must be weighed against the trauma of an investigation that may separate a child from parents who are otherwise loving and capable. Multicultural Therapy Competencies for Marriage and Family Therapists directly informs this work, as AAMFT ethics compel culturally competent practice that recognizes how systemic racism shapes both substance use trajectories and child welfare outcomes.2 Before filing a report, explore every alternative, consult with supervisors, and document the clinical rationale for any decision. The goal is to balance child safety with family preservation, centering the family's voice in the process.