Fewer than half of U.S. addiction treatment facilities offer couples programming.
IPV screening before any conjoint addiction session is non-negotiable.
Dual competency in relational therapy and substance use opens a high-demand MFT niche.
Federal health agencies report that millions of Americans who need addiction treatment never receive it, and among the key barriers is fear of partner separation during care.1 In June 2026, Couples Rehab in California expanded same-day admissions and insurance verification resources specifically for partners seeking treatment together, addressing a gap that MFTs routinely encounter in practice: clients ready for change but unwilling to enter individual programs that split them apart.
This guide is written for licensed and prelicensed marriage and family therapists who need a clinical playbook for couples-specific addiction work. It covers evidence-based models such as Behavioral Couples Therapy, structured screening protocols to rule out intimate partner violence, ethical guardrails around confidentiality and dual-client relationships, training pathways for couples therapists that add addiction credentials to systemic competencies, and referral protocols that coordinate care across disciplines.
Fewer than half of addiction treatment facilities in the United States offer programming designed for couples, and the shortage creates both a service gap and a professional opportunity for MFTs with dual training.
What Is Couples Rehab and How Does It Differ From Individual Treatment?
Fewer than half of addiction treatment facilities in the United States offer programming designed for couples, according to data from the Substance Abuse and Mental Health Services Administration. That scarcity matters, because couples rehab is not simply two people attending individual treatment at the same location. It is a distinct clinical model in which the relationship itself is treated as a unit, with shared goals, joint sessions, and coordinated recovery milestones woven into the treatment plan.
Defining Couples Rehab
Couples rehab refers to concurrent or conjoint addiction treatment in which both partners engage in a unified care plan. Therapists address substance use alongside relational dynamics: communication patterns, attachment injuries, enabling behaviors, and shared trauma. This stands apart from parallel individual treatment that happens to occur at the same time. In a true couples model, the therapeutic work explicitly targets the interaction between substance use and the relationship, rather than treating each partner in isolation and hoping the gains transfer.
Levels of Care Available to Couples
Couples can access addiction treatment across several levels of care, and MFTs should understand what each involves when making referrals.
Residential/inpatient: Partners live at the facility and receive 24-hour support, including medical detox if needed. Shared housing for couples is offered at select programs.
Partial hospitalization (PHP): Structured daytime programming (typically 20 or more hours per week) while couples return home in the evening.
Intensive outpatient (IOP): Usually 9 to 15 hours of weekly programming, allowing couples to maintain work or family responsibilities.
Standard outpatient: Weekly individual and conjoint sessions, often used as step-down care after a higher level of treatment.
Not all facilities accept couples together, and that logistical barrier can stall treatment at the exact moment motivation peaks. In June 2026, California-based Couples Rehab expanded its same-day admission resources, including insurance verification support and detox coordination, specifically to reduce the gap between a couple's decision to seek help and their entry into care.1 For MFTs, knowing which programs offer joint enrollment and rapid access is a practical referral advantage.
Signs a Couple Needs Rehab Together
Several clinical indicators suggest that treating partners jointly will produce better outcomes than sending each person to a separate program.
Co-using patterns where one partner's substance use reliably triggers or escalates the other's
Enabling dynamics that sustain active addiction, such as covering for a partner's absences or supplying substances
Relapse cycles driven by relational conflict, jealousy, or unresolved betrayal
Shared trauma histories, including experiences that both partners witnessed or endured together
When these patterns are present, treating one partner alone often fails because the relational system that maintains the addiction remains unchanged.
When Concurrent Treatment Beats an Individual-First Approach
Conventional wisdom sometimes holds that each partner should stabilize individually before attempting couples work. That sequence makes sense in certain cases, particularly when safety concerns exist. However, when substance use is deeply intertwined with attachment rupture or codependency, an individual-first approach can actually widen the emotional distance between partners and erode the motivation that brought them to treatment. In those situations, conjoint care allows clinicians to leverage the attachment bond as a recovery asset, reinforcing sobriety through relational repair rather than despite it. MFTs are uniquely positioned to make this clinical judgment because relational systems thinking and therapy modalities are at the core of their training.
Evidence-Based Couples Therapy Models for Addiction
Choosing an evidence-based approach for couples facing addiction means balancing the urgency of substance use treatment with the complexity of relational dynamics. While individual addiction counseling targets behavior change in one person, couples-focused models address the dyadic patterns that can either sustain use or support recovery. Understanding the core frameworks and knowing how to evaluate their fit for your clients will sharpen your clinical judgment and expand your referral repertoire.
Behavioral Couples Therapy (BCT)
Behavioral Couples Therapy is among the most widely researched interventions for substance use disorders in partnered populations. BCT integrates addiction-focused behavioral contracts (such as daily sobriety check-ins and disulfiram compliance agreements) with communication skills training and positive relationship-building exercises. The model operates on the premise that a stable, supportive partnership can reinforce abstinence and reduce relapse triggers. Studies published in peer-reviewed addiction and family therapy journals have consistently reported improvements in both substance use outcomes and relationship satisfaction when BCT is delivered alongside standard addiction treatment. MFTs interested in this approach should consult primary literature through PubMed, PsycINFO, and the websites of professional associations such as the American Association for Marriage and Family Therapy (AAMFT) and the Substance Abuse and Mental Health Services Administration (SAMHSA), which curate practice guides and systematic reviews.
Integrative Behavioral Couple Therapy (IBCT)
Integrative Behavioral Couple Therapy blends traditional behavior-change strategies with acceptance-based interventions. Rather than focusing solely on reducing substance use through contingency management, IBCT helps partners increase tolerance for differences, deepen emotional engagement, and reduce conflict that may trigger or perpetuate substance use. While IBCT was originally developed for general relationship distress, adaptations for addiction populations emphasize acceptance of the recovery process and the partner's role in creating a context for change. Clinicians can locate training manuals, workshops, and outcome data through university-affiliated therapy research centers and professional continuing-education platforms.
Emotionally Focused Therapy (EFT) and Systemic Approaches
Emotionally Focused Therapy, grounded in attachment theory, has been applied to couples coping with addiction by targeting the underlying emotional injuries and insecure attachment patterns that co-occur with substance dependence. EFT aims to restructure interactions so partners can serve as secure bases for one another during the stress of early recovery. Although the bulk of EFT research has centered on general relationship outcomes, emerging case studies and pilot trials suggest promise for addiction populations when combined with concurrent addiction services. Systemic family therapy models broaden the lens further, involving extended family members and examining multigenerational patterns of substance use. MFTs seeking training in these modalities should review offerings from the International Centre for Excellence in Emotionally Focused Therapy (ICEEFT) and explore family systems institutes that publish treatment fidelity measures and supervision resources.
Locating Current Evidence Yourself
To stay current, search databases such as Cochrane Reviews and the Journal of Marital and Family Therapy for meta-analyses comparing outcomes across models. When evaluating any model, look for studies that report both substance use metrics (days abstinent, relapse rates) and relational outcomes (satisfaction scores, intimate partner violence incidence) to ensure the approach addresses the full clinical picture your couples bring to treatment. Reviewing the therapy approaches used by MFTs can also help you map these addiction-focused models against the broader landscape of evidence-based couples modalities.
Questions to Ask Yourself
Does the relationship stabilize or destabilize their recovery?
A dynamic that reinforces use can erase individual treatment progress, even when both partners seek help together.
Is one partner coercing or controlling the other?
Conjoint therapy in an abusive dynamic risks escalating harm; safety must be assessed separately first.
Is both partners’ motivation genuine, or does the dynamic reinforce use?
Pressured participation can breed resistance, and enabling patterns may sustain addiction despite treatment.
When to Recommend, and When to Avoid, Couples Rehab
Referring a couple to conjoint addiction treatment versus recommending parallel individual work hinges on one overriding question: Is the relationship safe enough to support shared recovery, or does it amplify harm? The answer requires structured screening, clinical judgment, and a willingness to slow down intake when red flags emerge.
Screen for Intimate Partner Violence First, Always in Private
Before scheduling any conjoint session, conduct separate, individual interviews with each partner to screen for intimate partner violence. Use validated instruments to standardize your assessment. The Hurt, Insult, Threaten, Scream (HITS) tool is a four-item screener validated in primary care; a score of 10 or higher signals concern.1 The Danger Assessment, a 20-item instrument, evaluates lethality risk in abusive relationships and is particularly useful when you suspect escalating violence.2 Both tools carry sensitivity ranges between 26 and 87 percent and specificity from 80 to 97 percent in female populations, according to systematic reviews informing the U.S. Preventive Services Task Force 2024 grade B recommendation for IPV screening in women of reproductive age.3 The J-IPV, a four-item screener validated specifically in substance use disorder treatment settings as of 2023, offers a targeted option for addiction contexts.4
No validated IPV screening tools exist for male-identifying victims as of 2024, so supplement quantitative screens with open-ended clinical inquiry.1 The American College of Obstetricians and Gynecologists recommends screening at regular intervals, including new patient visits, annual exams, and prenatal encounters, in private, safe environments where the partner is not present.5 Apply that same privacy standard to every couples intake: screen individually before bringing the dyad into the room.
Absolute Contraindications: When Couples Therapy Is Unsafe
Conjoint addiction treatment is contraindicated in the presence of:6
Current severe or life-threatening intimate partner violence: Physical assault, strangulation, threats with weapons, or patterns that score high on the Danger Assessment.
Active protective orders: Legal separation for safety cannot coexist with therapeutic intimacy.
Severe coercive control: One partner uses substance supply, financial restriction, or isolation to dominate the other.
Ongoing substance use coercion: Forcing a partner to use, sabotaging recovery attempts, or threatening harm if the partner seeks help.
Acute psychiatric crisis in either partner: Active psychosis, imminent suicidal ideation, or untreated mania destabilizes the therapeutic frame.
When any of these conditions are present, refer each partner to separate providers and defer couples work until safety and psychiatric stability are achieved.
Gray Zones: Modified Couples Work with Safety Protocols
Not every instance of past or low-level conflict disqualifies a couple from conjoint treatment. Historical intimate partner violence that has resolved, with no incidents in the past year and demonstrated accountability by the formerly abusive partner, may permit carefully structured couples therapy. Gottman Method assessment tools can help gauge relational safety and motivation in these ambiguous cases. Mild situational couple violence, such as mutual shoving during arguments with no injury and no fear, can sometimes be addressed within the couples frame if both partners accept responsibility and agree to safety planning.
In these gray areas, proceed with caution:
Develop a written safety plan with both partners.
Schedule frequent individual check-ins to monitor for coercion or suppression.
Establish clear exit criteria if violence recurs.
Coordinate with a domestic violence advocate when appropriate.
Common MFT Errors: What Not to Do During Couples Therapy
Premature conjoint sessions are the most frequent mistake. Bringing an abusive partner and victim into shared space before safety is confirmed risks giving the abuser a therapeutic platform to manipulate, blame-shift, or intimidate. Treating the relationship before stabilizing individual safety reverses the necessary sequence of care. Other pitfalls include:
Assuming that both partners share equal motivation for recovery.
Neglecting to assess psychiatric comorbidity separately.
Failing to revisit safety screens as treatment progresses.
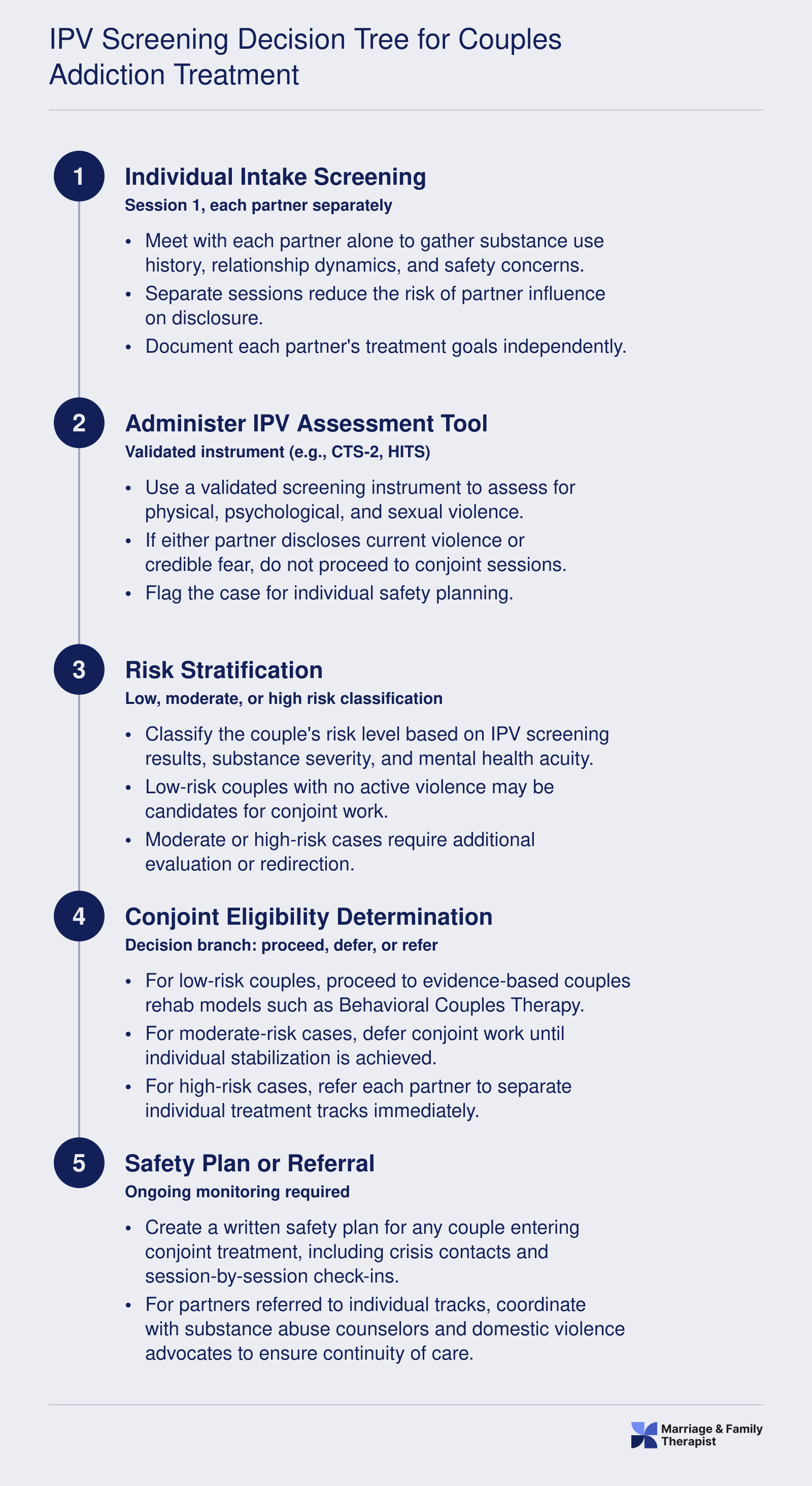
Use a clinical decision tree: screen for IPV individually, assess motivation symmetry and substance severity, confirm psychiatric stability, then decide whether to proceed conjointly or refer to parallel tracks. When in doubt, choose safety over speed.
IPV Screening Decision Tree for Couples Addiction Treatment
Before initiating any conjoint addiction work, MFTs must follow a structured screening protocol to identify intimate partner violence and determine whether couples rehab is clinically appropriate. Skipping or compressing these steps puts vulnerable clients at risk. Use this decision flow to guide every couples intake involving substance use.
Ethical and Legal Considerations for MFTs in Couples Addiction Work
How do you protect confidentiality when one partner discloses a relapse in an individual phone call, yet both remain your clients? That question sits at the heart of ethical practice in couples addiction therapy, where the boundaries of dual-client relationships, mandated reporting, and federal confidentiality protections intersect in ways that individual therapy simply does not encounter.
AAMFT Code of Ethics and Confidentiality in Conjoint Treatment
The AAMFT Code of Ethics governs your practice through eight core standards, with Standard II (Confidentiality) providing the clearest guidance for couples work.1 Sections 2.1 through 2.3 require you to explain the nature and limits of confidentiality early in the therapeutic relationship and obtain written authorization before disclosing any information.1 When treating couples, you must recognize that the couple is the client unit. Under the current code, you may not reveal individual confidences to others in that unit without prior written permission from the person who disclosed.1 This creates a direct tension: if Partner A tells you in a private message that they relapsed yesterday, you cannot share that information with Partner B without Partner A's written consent, even though both are your clients and the relapse may directly threaten the couple's recovery contract.
The No-Secrets Policy Debate
Most experienced couples addiction therapists resolve this tension by adopting a no-secrets policy at intake. You inform both partners, in writing, that any information shared individually (by phone, text, or sidebar conversation) will be brought into the joint session or the therapy will pause until the disclosure occurs. This policy must appear in your informed consent document, signed by both parties before the first session. The alternative, a limited-confidentiality model, allows individual secrets but often leads to therapeutic impasses: you cannot effectively treat the couple while holding material information asymmetrically. A no-secrets policy also reduces your liability if one partner later claims you concealed a relapse or endangered their safety by withholding critical facts.
Documentation and Dual-Client Records
When you treat a couple, your clinical record must reflect that the couple is the client. Chart notes should describe joint themes, not attribute every statement to one partner. If one partner drops out or files a complaint, the other remains your client, and you must continue protecting the confidentiality of both. Standard II requires that access to records not be provided without written authorization from each individual competent to execute a waiver.1 This means that if Partner A subpoenas your file, you cannot release it without Partner B's written consent, even if Partner A paid for the sessions. Your intake forms should include a joint records-release clause that both partners sign, authorizing each other to access records if separation or litigation occurs. MFT practice management software for couples and family therapy workflows can help you maintain compliant dual-client records and automate authorization tracking.
Mandatory Reporting and Duty to Warn
Addiction creates unique mandatory-reporting tensions. If a partner discloses impaired driving with children in the car, you face a duty to warn under Standard I (Responsibility to Clients) and state child-welfare statutes. That duty may override both AAMFT confidentiality protections and the stricter federal rules in 42 CFR Part 2.2 Part 2 applies to patient records of federally assisted substance use disorder programs and generally prohibits disclosure without specific written patient authorization.2 Subpoenas do not suffice under Part 2; a court order or valid authorization is required, and any authorization must include a redisclosure warning.2 If your practice receives any federal funding (Medicaid, Medicare, grants) and you provide SUD treatment, Part 2 likely applies. You must layer a Part 2-compliant consent form on top of your AAMFT informed consent, ensuring both partners authorize disclosures for coordination of care, billing, and mandated reports.1 When imminent danger exists, however, Part 2 permits disclosure to prevent death or serious harm without authorization, aligning with your ethical duty to warn.
State Scope-of-Practice Variations
Not every state grants MFTs full authority to treat substance use disorders independently. Some jurisdictions require an additional SUD credential, co-supervision by a licensed addiction counselor, or registration as a SUD provider before you can bill for or advertise addiction-focused couples therapy. Before marketing yourself as a couples addiction specialist, verify your state board's scope rules and secure any required endorsements. You can review addiction therapist licensure requirements to understand how SUD credentials intersect with MFT scope across states. If your scope is limited, establish a co-treatment or referral relationship with a licensed SUD professional to ensure compliance and continuity of care.
Establish a written confidentiality policy before the first conjoint session: it is non-negotiable. Ambiguity about how you will handle secrets creates serious clinical and legal exposure the moment one partner privately discloses active substance use. Decide your no-secrets stance in advance, put it in your informed consent, and have both partners sign before addiction content ever enters the room.
Structuring Treatment: From Intake Assessment to Aftercare Planning
Couples who enter addiction treatment together are statistically more likely to complete the program than those who enter alone, a finding consistent across multiple clinical trials of behavioral couples therapy. That retention advantage is real, but it depends entirely on having a coherent, phase-based structure that adapts as the couple moves through levels of care.
Phase 1: Stabilization and Early Psychoeducation
The first priority after intake is safety, not conjoint work. During detox and early residential stabilization, individual medical management and psychiatric assessment take precedence. The MFT's role in this phase is to engage both partners separately, conduct thorough individual histories, and begin family psychoeducation. Partners who are not in detox themselves need support understanding withdrawal timelines, what to expect behaviorally, and how enabling patterns may have developed. Conjoint sessions at this stage are generally contraindicated until the substance-using partner has achieved medical stability.
Phase 2: Active Treatment and Introducing Couples Sessions
Once stabilization is complete, the couple track can open alongside individual SUD work. Session frequency should match the level of care:
Residential: Daily group programming plus two to three conjoint couples sessions per week, focused on communication repair and early trust rebuilding.
Intensive outpatient (IOP): One couples session per week coordinated alongside three group sessions per week, shifting toward relapse-prevention skill building as a unit.
Standard outpatient: Weekly or biweekly couples sessions, with flexibility to increase frequency during high-risk periods.
During this phase, coordinate actively with the prescribing physician or psychiatrist. If a partner is on medication-assisted treatment (MAT) such as buprenorphine or naltrexone, the couples therapist should be looped into the treatment team so that session goals align with the medical timeline. Psychiatric medications for co-occurring conditions require the same coordination. The couple therapist is not managing prescriptions, but understanding the medication context shapes how sessions are framed and paced.
Couple-Based Relapse Prevention Protocols
The clinical core of Phase 2 and the bridge into Phase 3 involves structured relapse prevention work designed for two people rather than one. Useful protocols include:
Sobriety contracts: Written agreements that specify what each partner will do, and ask of the other, to support abstinence. These are collaborative, not punitive.
Joint trigger mapping: Both partners identify environmental, emotional, and relational cues that have historically preceded use. Mapping these together reduces concealment and builds shared awareness.
Trust-rebuilding behavioral exchanges: Borrowed from emotionally focused therapy principles, these are concrete, daily positive actions each partner agrees to perform, creating momentum separate from the crisis of addiction.
Communication scripts for high-risk moments: Rehearsed phrases and agreed-upon time-out procedures that give couples a plan when tension escalates instead of improvising under pressure.
Phase 3: Maintenance, Aftercare, and Community Integration
Discharge planning should begin well before the final session, not at it. Step-down criteria typically include demonstrated sobriety stability, reduced conflict frequency, and at least partial restoration of trust behaviors identified in treatment. Transition goals should be documented in writing and shared with the receiving outpatient provider.
Community referrals matter here. Mutual-aid options specifically designed for couples, such as Recovering Couples Anonymous, give partners a peer community that reinforces the relational recovery frame rather than routing them into separate programs that can inadvertently pull them apart. Referrals to individual sponsors or groups remain appropriate alongside couples-specific resources, not instead of them.
Discharge is a handoff, not a finish line. The aftercare plan should name the next provider, confirm the first appointment before the client leaves, and include a written crisis protocol the couple has reviewed together.
Training, Credentials, and Career Pathways for MFTs in Addiction
Marriage and family therapists who build dual competency in relational dynamics and substance use disorders occupy a rare and strategically valuable niche in behavioral health. Unlike most addiction counselors who lack systemic training, and unlike many LMFTs who refer out the moment substance use surfaces, MFTs with addiction credentials can treat the couple and the disorder in tandem.
The Educational Foundation
Every MFT addiction career begins with a COAMFTE accreditation-backed master's program. Accreditation standards require all MFT curricula to include coursework in substance abuse and addictive disorders, covering procedures for identifying substance use, addiction, and co-occurring disorders within a systemic framework.1 Programs like Lipscomb University's COAMFTE-accredited track ensure that graduates complete at least 300 clinical hours and receive foundational exposure to SUD assessment and treatment planning.2 After graduation, candidates must accumulate state-mandated postgraduate hours (Tennessee, for example, requires 1,000 hours3) before sitting for the national MFT licensing exam and earning LMFT status.
Adding Addiction Credentials
Once licensed, MFTs can pursue state-level substance use disorder credentials that expand billing opportunities and scope of practice. States issue endorsements such as Licensed Alcohol and Drug Counselor (LADC), Certified Alcohol and Drug Counselor (CADC), or Licensed Chemical Dependency Counselor (LCDC).4 These credentials are open to LMFTs and typically require a combination of supervised SUD-specific clinical hours, coursework, and a state examination. Holding both an LMFT license and a state SUD credential signals dual expertise to employers, insurers, and referral sources. For a closer look at how dual certification LMFT and CADC pathways compare to other addiction counselor routes, the distinction matters most when negotiating scope of practice with employers.
The American Association for Marriage and Family Therapy does not currently offer a formal addiction specialty certification, but it does provide continuing education on substance use disorders, co-occurring disorders, and systemic approaches to addiction.5 MFTs also pursue post-graduate certificates and agency-based training in evidence-based models like Behavioral Couples Therapy, though no centralized AAMFT-recognized BCT institute directory exists as of 2026.5
Market Differentiation and Career Settings
MFTs with addiction credentials work across private practice, residential treatment facilities, hospital-based programs, and integrated behavioral health clinics. This versatility translates into varied compensation. Dual-credentialed clinicians can also pursue AAMFT-approved supervisor status, positioning themselves to train the next generation of addiction-competent MFTs and earn additional income through supervision fees. To explore the full range of settings and roles available, MFT career paths offer context on how specialization shapes long-term earning potential.
MFT Salary Snapshot: National and Top-Paying States
Understanding earning potential helps MFTs evaluate whether specializing in couples addiction work is financially viable. The table below draws from the most recent Occupational Employment and Wage Statistics published by the U.S. Bureau of Labor Statistics (2024 data). States with the highest mean annual wages for marriage and family therapists include Connecticut, Oregon, and New Jersey, though median pay can vary significantly depending on local demand and cost of living.
State
Total Employment
Mean Annual Wage
25th Percentile
Median Annual Wage
75th Percentile
Connecticut
390
$94,830
$59,000
$76,930
$138,610
Oregon
1,080
$94,520
$65,400
$79,890
$137,950
New Jersey
3,940
$91,980
$77,380
$89,030
$97,670
Colorado
810
$89,280
$54,960
$69,990
$104,990
Utah
1,980
$85,550
$63,220
$81,170
$102,810
Maryland
340
$84,900
$58,560
$65,300
$113,800
Virginia
910
$78,900
$54,010
$80,670
$95,120
Ohio
710
$78,300
$41,600
$63,880
$96,220
California
32,070
$74,660
$47,730
$63,780
$91,660
Minnesota
3,780
$72,900
$59,720
$72,370
$82,870
Iowa
90
$72,070
$49,460
$61,450
$71,030
Missouri
530
$70,010
$51,310
$64,900
$80,760
New Mexico
250
$68,660
$57,800
$67,990
$76,070
Massachusetts
530
$68,430
$56,720
$62,290
$81,810
Pennsylvania
2,360
$67,940
$55,580
$64,570
$80,100
Interdisciplinary Collaboration and Referral Resources
Effective couples addiction treatment rarely happens in a single silo. Interdisciplinary collaboration means intentionally weaving together multiple providers so that each element of a couple's recovery gets expert attention, while keeping the relational work central. For MFTs, this isn't about handing off the addiction piece; it's about orchestrating a team that respects the couple's systemic dynamics.
Assembling the Core Treatment Team
A well-rounded team typically includes: the MFT leading relational and systemic interventions; an addiction counselor delivering individual substance use sessions; a psychiatrist or prescriber managing medication-assisted treatment (MAT) or co-occurring mental health medications; a case manager handling benefits, housing, or legal barriers; and a primary care provider for overall health monitoring. The MFT's role is unique: you track how each of these services influences the relationship and vice versa. For example, if MAT reduces cravings but one partner feels the other is "replacing one drug with another," that relational ripple must be addressed in session.
Building a Referral Network with Couples-Specific Programs
Not all addiction programs are designed for couples. When seeking referral partners, look for facilities that offer simultaneous intake, coordinated treatment plans, and a philosophy that views the relationship as a potential recovery asset rather than a distraction. As a benchmark, consider the recent expansion of same-day admission and insurance verification resources by Couples Rehab, which specifically targets married couples and committed partners facing substance use challenges together.1 This model illustrates what MFTs should prioritize in a referral: the ability to move quickly when a couple is ready, minimal separation anxiety through joint programming, and administrative support that reduces drop-off between initial motivation and actual admission. Build a vetted list of programs that can provide detox coordination, dual-diagnosis capacity, and aftercare planning aligned with your therapy goals.
Mastering the Warm Handoff: Information Sharing and Coordination
A warm handoff goes beyond a phone number. Start by obtaining a release of information that respects 42 CFR Part 2 confidentiality rules for substance use treatment. Then share a concise clinical summary: relationship strengths and vulnerabilities, substance use patterns, any safety concerns, and your current treatment goals. Avoid raw therapy notes; instead, highlight what the addiction team needs to know to avoid unintended triangulation. Coordinate by scheduling brief joint case reviews, and when disagreements arise, frame them as opportunities for richer formulation. For instance, if the addiction counselor insists on individual work before couples sessions, explore the rationale together, adjusting the overall plan without undermining either provider.
Knowing When to Refer Out Entirely
MFTs must recognize the boundary of their competence. Refer out when the couple requires a higher level of care (inpatient detoxification, residential treatment), when medical or psychiatric complexity exceeds your training, or when active intimate partner violence makes couples work contraindicated. In such cases, stabilize safety first, then maintain a supportive role as the treatment team re-engages the couple once the acute phase passes. For MFTs weighing how this specialty fits their broader practice, exploring MFT career paths can help clarify where addiction-focused couples work fits within the profession.
Questions to Ask Yourself
Have you completed formal training in at least one evidence-based couples addiction model?
Structured model training ensures you address the addiction-relationship cycle, not just communication. Generic couples work risks overlooking substance use triggers within the partnership.
Do you have a written confidentiality policy for conjoint substance use disorder sessions?
A policy pre-commits both partners to clear limits, preventing ethical dilemmas when one reveals ongoing use that could harm the other.
Do you maintain a current referral list of couples-accepting treatment programs in your area?
An updated list prevents treatment delays and ensures couples receive coordinated care, rather than separate programs that might conflict with relationship-based goals.
Cultural Competence, LGBTQ+ Considerations, and Telehealth Adaptations
What cultural, LGBTQ+, and telehealth adaptations are needed when treating couples with substance use disorders? Clinicians must weave cultural humility, inclusive practices, and virtual delivery modifications into every phase of care. Behavioral Couples Therapy (BCT) is a well-established model with 12, 20 sessions over 3, 6 months, showing reductions in substance use and intimate partner violence across dozens of RCTs.1 But its effectiveness hinges on tailoring to each couple's identities and context, especially as telehealth becomes a permanent care modality.
Cultural Humility in Couples Addiction Treatment
Substance use stigma varies widely across cultures, shaping whether partners seek help. Gender role expectations can silence the partner who uses substances or cast blame on the non-using partner, disrupting the collaborative stance BCT requires. MFTs should assess family-of-origin attitudes toward addiction and help-seeking early in treatment. For example, in collectivist cultures, the couple may prioritize saving face over disclosure, so clinicians can reframe treatment as a shared commitment to family well-being rather than an individual failing. Avoid universalizing Western concepts of addiction as a disease , explore the couple's own explanatory model and integrate their language.
LGBTQ+ Considerations in Couples Rehab
LGBTQ+ couples face elevated minority stress, a documented relapse risk factor. Internalized stigma, family rejection, and past discrimination in healthcare can compound relational distress and substance use. Intake forms must use inclusive language for relationship status, pronouns, and sexual orientation. Treatment materials should depict diverse couples. Beyond surface inclusivity, MFTs need to address how heterosexism may have shaped the couple's substance use patterns. For instance, a partner's heavy drinking at a gay bar might be both a social lifeline and a trigger. Resources on LGBTQ+ affirming mental health care can help clinicians identify affirming referral networks and build culturally responsive treatment plans. Navigating family rejection requires balancing the couple's need for autonomy with the benefits of social support , clinicians can help them build chosen family networks.
Telehealth Adaptations for Behavioral Couples Therapy
Emerging evidence shows that Alcohol Behavioral Couples Therapy (ABCT) delivered virtually yields comparable outcomes to in-person treatment.2 Telehealth SUD treatment overall has permanent Medicare and Medicaid coverage, with retention for medication-assisted treatment non-inferior to in-person.3 Couple and family therapy for SUD consistently outperforms individual or group modalities.4 For BCT, psychoeducation about the recovery contract, behavioral contracts, and structured daily check-ins translate smoothly to video. The therapeutic alliance remains strong on video platforms.3 However, safety monitoring for intimate partner violence (IPV) is harder , non-verbal cues are partial, and a controlling partner may surveil the session. When IPV history is present, clinicians must require separate physical spaces and screens; if safety cannot be assured, shift to individual check-ins before reuniting the couple.
Practical Telehealth Guidelines for High-Risk Couples
SAMHSA and AAMFT telehealth toolkits emphasize risk screening, confidentiality, and digital boundaries.5 For couples with SUD and IPV risk: mandate separate rooms and devices; ask safety-check questions via chat or text before conjoint parts; use a platform compliant with 42 CFR Part 2 for SUD records if billing electronically. State licensure portability remains a barrier , MFTs must verify they are authorized to treat clients in the state where the couple sits during each session. Document the physical location each time. Despite these challenges, telehealth expands access for rural or homebound couples, making it a vital option when cultural, sexual minority, or logistical barriers block in-person care.
Frequently Asked Questions About Couples Rehab for MFTs
These are among the most common questions marriage and family therapists ask when considering couples rehab as a treatment pathway for clients facing co-occurring addiction. Each answer draws on established models, ethics codes, and clinical best practices to help you navigate this specialized area of practice with confidence.
Can married couples go to rehab together?
Yes. Many residential and outpatient programs now accept married couples and committed partners for concurrent treatment. A California-based organization, Couples Rehab, expanded its same-day admissions resources in June 2026, specifically targeting partners who want to enter treatment together. Programs like these coordinate detox, insurance verification, and joint programming so couples do not have to separate to receive care.
How does behavioral couples therapy (BCT) work for substance abuse?
BCT pairs abstinence-focused behavioral contracts with relationship skill building. Both partners agree to a daily "Recovery Contract" that includes a sobriety commitment, witnessed medication compliance if applicable, and positive verbal reinforcement. Sessions then layer in communication training, problem-solving exercises, and shared activity scheduling. Research consistently shows BCT reduces substance use and improves relationship satisfaction more effectively than individual treatment alone.
When is couples rehab contraindicated due to domestic violence?
Couples rehab should be avoided whenever active intimate partner violence (IPV) is present and the victimized partner's safety cannot be assured. Use a validated screening tool such as the Conflict Tactics Scale (CTS-2) or the Danger Assessment at intake. The AAMFT Code of Ethics requires practitioners to prioritize client safety. If coercive control, stalking, or physical violence is identified, refer each partner to individual services before considering any conjoint format.
What training do MFTs need to treat couples with addiction?
At minimum, MFTs should pursue graduate-level coursework or continuing education in substance use disorders, co-occurring mental health diagnoses, and evidence-based models like BCT or the Community Reinforcement and Family Training (CRAFT) approach. Many states accept NAADAC or IC&RC certifications as supplemental credentials. The AAMFT recommends ongoing supervision in addiction-specific cases, and some employers prefer candidates who hold both an LMFT license and a substance abuse counseling credential.
What are the signs a couple needs rehab rather than standard couples therapy?
Key indicators include one or both partners using substances daily or nearly daily, failed prior attempts at outpatient treatment, escalating relational conflict driven by substance use, co-occurring mental health crises, and physical withdrawal risk that requires medical supervision. When substance use is so pervasive that it undermines the couple's ability to engage meaningfully in weekly therapy sessions, a structured rehab program with integrated couples work becomes the more appropriate level of care.
How do MFTs handle confidentiality when one partner relapses during conjoint treatment?
This scenario must be addressed proactively at intake through a clear informed consent and a "no secrets" policy or a defined disclosure protocol. The AAMFT Code of Ethics (Standard 2.2) requires therapists to clarify the limits of confidentiality with all parties at the outset. If a relapse is disclosed privately, the therapist follows the protocol the couple agreed to, which typically involves encouraging voluntary disclosure within a set timeframe or pausing conjoint sessions until safety and honesty can be reestablished.