MFT Internship Vs. Practicum Vs. Traineeship: Key Differences
If you have spent any time researching MFT clinical experience requirements, you have probably noticed that programs, state boards, and accrediting bodies do not always use the same vocabulary. The terms practicum, internship, traineeship, and fieldwork can overlap or mean entirely different things depending on who is doing the defining. Getting clear on these distinctions early will save you confusion later, especially when you need to document hours for licensure.
Practicum: Your First Clinical Exposure
A practicum is typically the earliest hands-on component of an MFT program. During this phase, you may observe experienced clinicians, co-facilitate sessions, or carry a small caseload under close supervision. Think of it as a structured introduction to clinical work rather than a deep immersion. In Texas, the state licensing board frames the practicum as a formal academic requirement of nine semester hours, four quarter hours, or 12 months of supervised practice.1 New York similarly references a "supervised practicum or internship" as the pre-degree clinical component and requires at least 300 direct client contact hours before graduation.1 Florida groups practicum, internship, and field experience together, requiring a minimum of 400 direct client contact hours.2
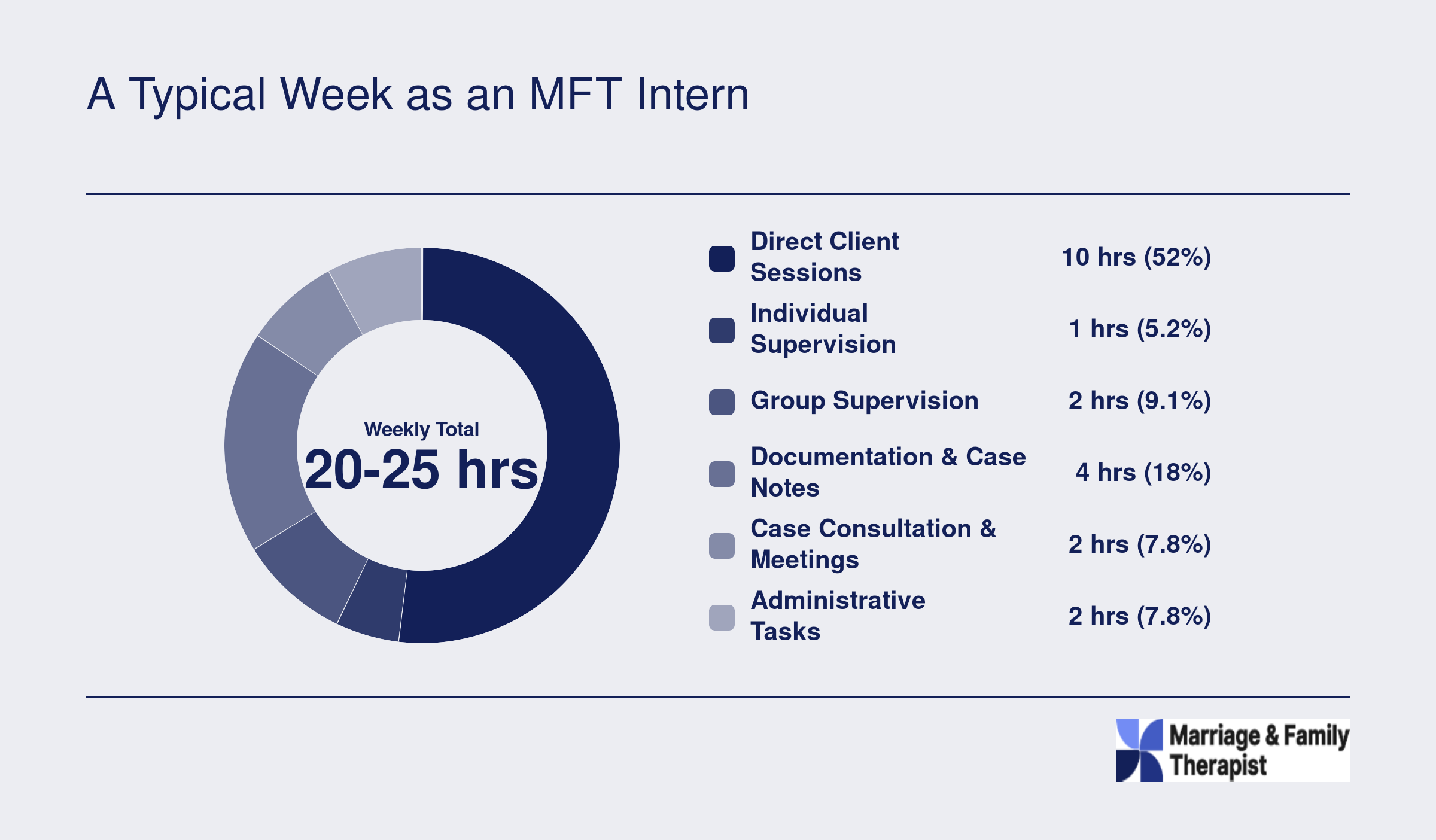
Internship: Intensive, Direct Client Work
The internship usually follows the practicum and represents the most intensive clinical stage of your master's program. You carry a larger caseload, take greater responsibility for treatment planning, and build the skills that will define your early professional identity. Programs accredited by COAMFTE require a minimum of 300 direct client contact hours across the full clinical training sequence, though many programs exceed that threshold.3 If you are still comparing masters MFT programs, pay close attention to how each one structures and labels these clinical phases.
Traineeship: A State-Specific Label
Some states use the word "traineeship" to describe pre-degree clinical work. California is the most prominent example. The California Board of Behavioral Sciences defines a trainee as someone currently enrolled in a qualifying graduate program who is gaining clinical experience, with a minimum of 150 face-to-face client contact hours required during that period.4 Once you graduate and register with the board, your title shifts from trainee to associate, and the hour-counting rules change. If your state does not use the traineeship label, you likely will not encounter it in your own licensing paperwork.
Fieldwork: The Umbrella Term
Many programs use "fieldwork" as a catch-all that covers both practicum and internship phases. Whether your program handbook says fieldwork, clinical placement, or something else, what matters is understanding which specific hours count toward your state board's requirements and which count toward your program's graduation standards. These two sets of requirements often overlap but are not always identical.
Why the Terminology Matters for You
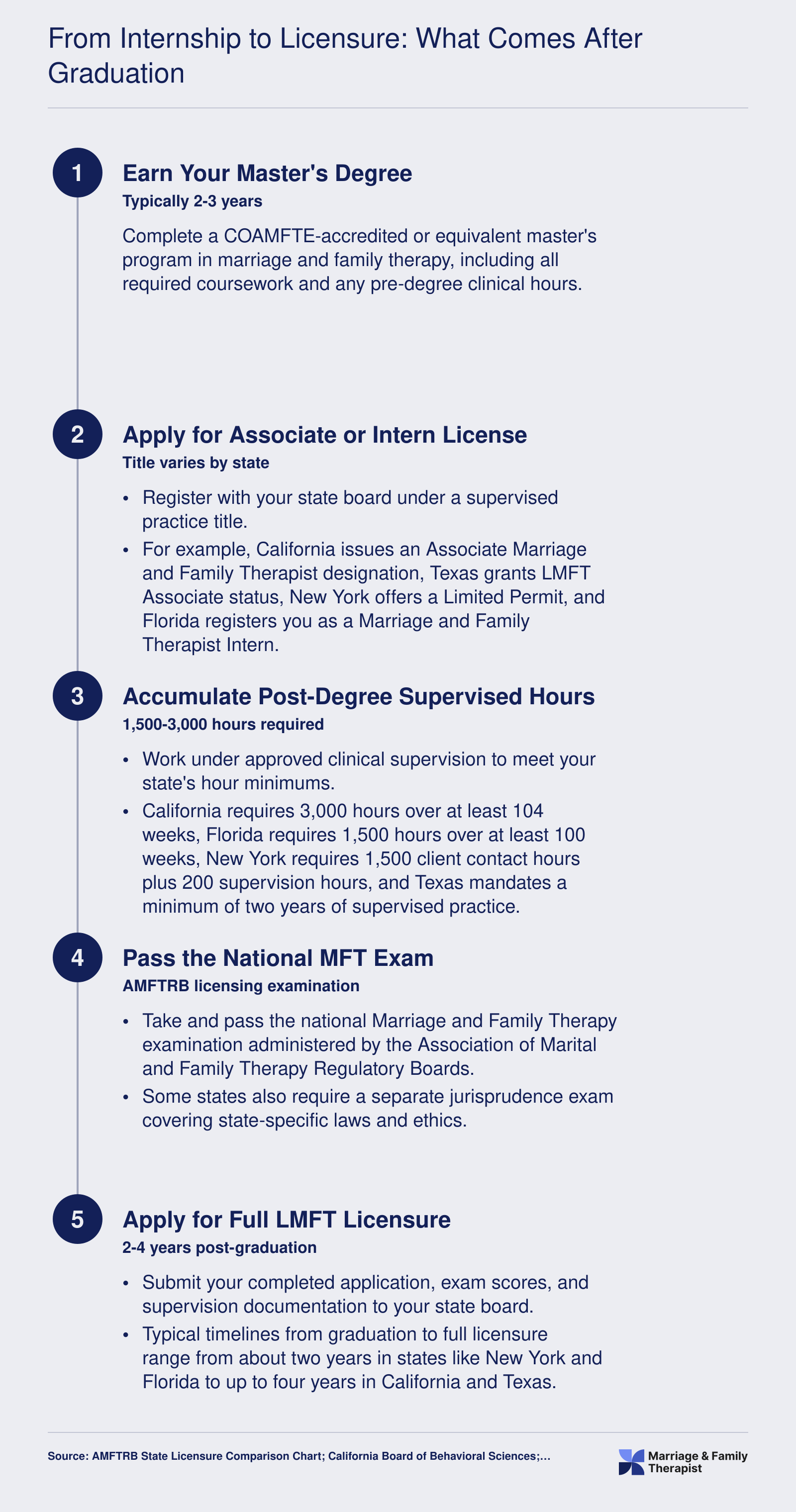
Accrediting bodies and state boards do not always speak the same language. COAMFTE's standards describe a foundational practice component with specific hour minimums, while AAMFT does not formally define pre-degree clinical work in the same way, focusing instead on post-degree requirements such as 1,000 client contact hours and 200 supervision hours for its Approved Supervisor designation.5 Your state licensing board, meanwhile, may use its own terminology and set its own hour thresholds. For a broader look at how these requirements fit into the full path toward practice, review our guide to becoming an MFT.
The practical step here is straightforward: look up the exact terms your program and your state board use, then create a simple tracking document that maps your completed hours to both sets of requirements. If you plan to practice in a different state from where you attend school, check that state's definitions as well. Knowing precisely what each authority calls each stage of your training, and what counts under each label, keeps you from discovering a shortfall at the worst possible time.